Surgical Treatment of Undisplaced Femur Neck Fractures in Dementia Patients Using Proximal Femoral Nail Antirotation
- Affiliations
-
- 1Department of Orthopedic Surgery, Gwangju Veterans Hospital, Gwangju, Korea. chm1228@hanmail.net
- KMID: 2069146
- DOI: http://doi.org/10.5371/hp.2015.27.3.164
Abstract
- PURPOSE
People with dementia have poor mobility and discharge outcomes following hip fractures. The purpose of this study was to evaluate the clinical and radiological results of internal fixation of undisplaced femur neck fractures (Garden types 1 and 2) by proximal femoral nail antirotation (PFNA) in dementia patients.
MATERIALS AND METHODS
We studied retrospectively 19 patients with undisplaced femur neck fracture. All patients were over 70 years of age, walked independently with a cane or crutches and suffered moderate-to-severe dementia. Patients were treated with PFNA and followed-up for more than 2 years. Revision, loss of fixation, complications, and walking ability outcomes were measured.
RESULTS
In walking-ability evaluation, patients showed an average decrease of just 0.2 points at the final follow-up. Walking ability was evaluated from before injury to 4 weeks after surgery and decreased by less than 0.5 points. Radiological bone union was achieved in 17 cases; the average time to bone union was 4.14 months (range, 2.5-7 months). Complications included non-union in two cases and femoral head avascular necrosis in one case of non-union.
CONCLUSION
We found that for patients with osteoporotic bone tissues in their femoral heads or patients (e.g., those suffering dementia) for whom cooperating with medical workers for postoperative walking control or rehabilitation exercises is difficult, implanting a mechanically stable spiral blade for fixation of femoral neck fractures could facilitate walking after surgery.
MeSH Terms
Figure
-
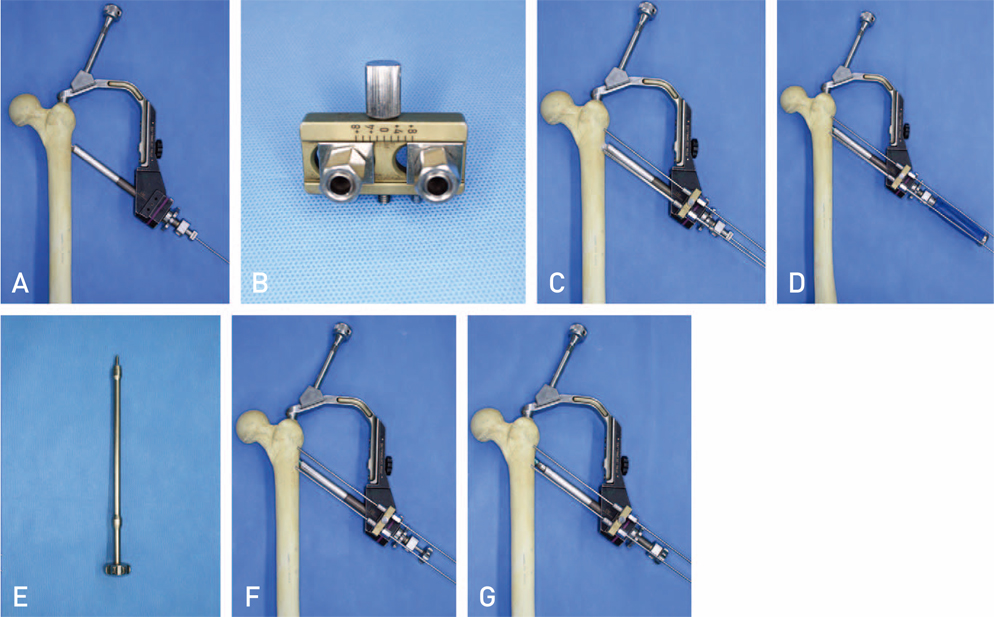
Fig. 1 (A) A guide wire was inserted into the center of the femoral head. (B) The aiming zig for antirotation wire. (C) The aiming zig for antirotation wire was attached to the buttress nut and 2 antirotation wires were inserted into the femoral head. (D) A helical blade was inserted into the femoral head. (E) The compression instrument for the proximal femoral nail antirotation blade. (F) The compression instrument was attached to the blade and intraoperative compression was obtained over the buttress nut and the protection sleeve. (G) After compression using the compression instrument.

Fig. 2 An 82-year-old male patient with a femoral neck fracture was treated with the proximal femoral nail antirotation. (A) Pre-operative radiograph showing an undisplaced femoral neck fracture. (B) Radiograph at the final follow-up (34 months after surgery) showing solid union without any evidence of mechanical failure. (C) Magnetic resonance image showing complete union at the fracture site and no evidence of avascular necrosis of the femoral head. (D) 99mTc-hydroxymethane diphosphonate bone single-photon-emission computed tomography showing radiotracer uptake in the femoral head suggestive of femoral head viability.
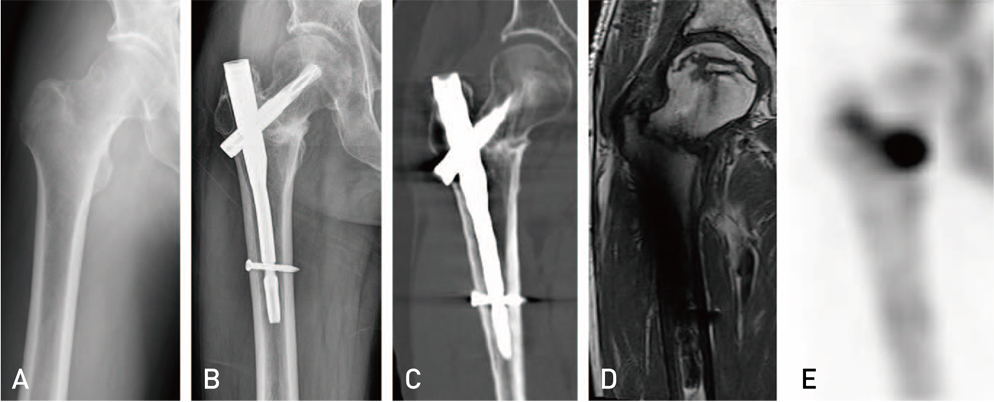
Fig. 3 A 75-year-old male patient with a femoral neck fracture was treated with the proximal femoral nail antirotation (PFNA). (A) Pre-operative radiograph showing an undisplaced femoral neck fracture. (B) PFNA fixation performed within 24 hours of injury, and a radiograph showing a sclerotic change at the fracture site 18 months after surgery. (C) Computed tomographic radiograph 18 months after surgery showing a sclerotic change at the fracture site and suggesting non-union. (D) Necrotic zone located in the superior aspect of the femoral head on a mid-coronal image. (E) 99mTc-hydroxymethane diphosphonate bone single-photon-emission computed tomography showing no radiotracer uptake, suggestive of avascular necrosis of the femoral head.
Reference
-
1. Garden RS. Stability and union in subcapital fractures of the femur. J Bone Joint Surg Br. 1964; 46:630–647.
Article2. Gjertsen JE, Engesaeter LB, Furnes O, et al. The Norwegian Hip Fracture Register: experiences after the first 2 years and 15,576 reported operations. Acta Orthop. 2008; 79:583–593.
Article3. Rogmark C, Flensburg L, Fredin H. Undisplaced femoral neck fractures--no problems? A consecutive study of 224 patients treated with internal fixation. Injury. 2009; 40:274–276.
Article4. Leighton RK, Schmidt AH, Collier P, Trask K. Advances in the treatment of intracapsular hip fractures in the elderly. Injury. 2007; 38:Suppl 3. S24–S34.
Article5. Lin D, Lian K, Ding Z, Zhai W, Hong J. Proximal femoral locking plate with cannulated screws for the treatment of femoral neck fractures. Orthopedics. 2012; 35:e1–e5.
Article6. Mir HR, Edwards P, Sanders R, Haidukewych G. Results of cephallomedullary nail fixation for displaced intracapsular femoral neck fractures. J Orthop Trauma. 2011; 25:714–720.
Article7. Chen WC, Yu SW, Tseng IC, Su JY, Tu YK, Chen WJ. Treatment of undisplaced femoral neck fractures in the elderly. J Trauma. 2005; 58:1035–1039.
Article8. Heyse-Moore GH. Fixation of intracapsular femoral neck fractures with a one-hole plate dynamic hip screw. Injury. 1996; 27:181–183.
Article9. Watson A, Zhang Y, Beattie S, Page RS. Prospective randomized controlled trial comparing dynamic hip screw and screw fixation for undisplaced subcapital hip fractures. ANZ J Surg. 2013; 83:679–683.
Article10. Asnis SE, Wanek-Sgaglione L. Intracapsular fractures of the femoral neck. Results of cannulated screw fixation. J Bone Joint Surg Am. 1994; 76:1793–1803.
Article11. Bliemel C, Lechler P, Oberkircher L, et al. Effect of preexisting cognitive impairment on in-patient treatment and discharge management among elderly patients with hip fractures. Dement Geriatr Cogn Disord. 2015; 40:33–43.
Article12. Koval KJ, Skovron ML, Aharonoff GB, Meadows SE, Zuckerman JD. Ambulatory ability after hip fracture. A prospective study in geriatric patients. Clin Orthop Relat Res. 1995; (310):150–159.13. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975; 12:189–198.14. Owens WD, Felts JA, Spitznagel EL Jr. ASA physical status classifications: a study of consistency of ratings. Anesthesiology. 1978; 49:239–243.15. Cleveland M, Bosworth DM, Thompson FR, Wilson HJ Jr, Ishizuka T. A ten-year analysis of intertrochanteric fractures of the femur. J Bone Joint Surg Am. 1959; 41-A:1399–1408.
Article16. Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995; 77:1058–1064.
Article17. Alho A, Benterud JG, Solovieva S. Internally fixed femoral neck fractures. Early prediction of failure in 203 elderly patients with displaced fractures. Acta Orthop Scand. 1999; 70:141–144.
Article18. Arnold WD, Lyden JP, Minkoff J. Treatment of intracapsular fractures of the femoral neck. With special reference to percutaneous Knowles pinning. J Bone Joint Surg Am. 1974; 56:254–262.19. Ficat RP. Idiopathic bone necrosis of the femoral head. Early diagnosis and treatment. J Bone Joint Surg Br. 1985; 67:3–9.
Article20. Bray TJ, Smith-Hoefer E, Hooper A, Timmerman L. The displaced femoral neck fracture. Internal fixation versus bipolar endoprosthesis. Results of a prospective, randomized comparison. Clin Orthop Relat Res. 1988; (230):127–140.21. Lu-Yao GL, Keller RB, Littenberg B, Wennberg JE. Outcomes after displaced fractures of the femoral neck. A meta-analysis of one hundred and six published reports. J Bone Joint Surg Am. 1994; 76:15–25.
Article22. Chang JS, Shon WY, Shin HC, Chae DJ, Lee SH. A clinical study of treatment of displaced fractures of femur neck with internal fixation in elderly patients. J Korean Orthop Assoc. 1992; 27:131–138.
Article23. Swiontkowski MF, Harrington RM, Keller TS, Van Patten PK. Torsion and bending analysis of internal fixation techniques for femoral neck fractures: the role of implant design and bone density. J Orthop Res. 1987; 5:433–444.
Article24. Windolf M, Braunstein V, Dutoit C, Schwieger K. Is a helical shaped implant a superior alternative to the Dynamic Hip Screw for unstable femoral neck fractures? A biomechanical investigation. Clin Biomech (Bristol, Avon). 2009; 24:59–64.
Article25. Vidyadhara S, Rao SK. Cephalomedullary nails in the management of ipsilateral neck and shaft fractures of the femur--one or two femoral neck screws? Injury. 2009; 40:296–303.
Article26. Zlowodzki M, Jönsson A, Paulke R, Kregor PJ, Bhandari M. Shortening after femoral neck fracture fixation: is there a solution? Clin Orthop Relat Res. 2007; 461:213–218.27. Boraiah S, Paul O, Gardner MJ, et al. Outcomes of length-stable fixation of femoral neck fractures. Arch Orthop Trauma Surg. 2010; 130:1523–1531.
Article28. Lee KJ. Fixation failure of proximal femoral nail antirotation in femoral intertrochanteric fracture. Hip Pelvis. 2012; 24:302–308.
Article29. Pui CM, Bostrom MP, Westrich GH, et al. Increased complication rate following conversion total hip arthroplasty after cephalomedullary fixation for intertrochanteric hip fractures: a multi-center study. J Arthroplasty. 2013; 28:8 Suppl. 45–47.
Article30. Bercik MJ, Miller AG, Muffly M, Parvizi J, Orozco F, Ong A. Conversion total hip arthroplasty: a reason not to use cephalomedullary nails. J Arthroplasty. 2012; 27:8 Suppl. 117–121.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Femoral Intertrochanteric Fracture with Proximal Femoral Nail
- Excessive Sliding of the Helical Blade and the Femoral Neck Fracture after Insertion of Proximal Femoral Nail Anti-Rotation for Type A2 Intertrochanteric Fractures - A Case Report -
- Treatment of the Proximal Femoral Extracapsular Fracture with Proximal Femoral Nail Antirotation (PFNA): Comparison with Proximal Femoral Nail (PFN)
- Results of the Proximal Femoral Nail-Antirotation (PFNA) in Patients with an Unstable Pertrochanteric Fracture
- The Determination of Optimal Entry Point for Proximal Femoral Nail Antirotation-II by Fluoroscopic Simulation: A Cadaveric Study
