A Potential Echocardiographic Classification for Constrictive Pericarditis Based on Analysis of Abnormal Septal Motion
- Affiliations
-
- 1Department of Cardiology, Waikato Hospital, Hamilton, New Zealand. dilesh@heartcarecentre.co.nz
- 2Department of Cardiology, Khoo Teck Puat Hospital, Singapore.
- 3Department of Cardiothoracic Surgery, Waikato Hospital, Hamilton, New Zealand.
- 4Department of Cardiology, Royal Prince Alfred Hospital, Sydney, Australia.
- KMID: 2068724
- DOI: http://doi.org/10.4250/jcu.2015.23.3.143
Abstract
- BACKGROUND
Constrictive pericarditis is an uncommon condition that could be easily confused with congestive heart failure. In symptomatic patients, septal "wobble" on echocardiography may be an important sign of constrictive physiology. This study was planned to investigate the effects of constriction on septal motion as identified by echocardiography.
METHODS
In this retrospective observational study, nine consecutive patients with constriction underwent careful echocardiographic analysis of the interventricular septum (IVS) with slow motion 2-dimensional echocardiography and inspiratory manoeuvres. Six patients who had undergone cardiac magnetic resonance imaging underwent similar analysis. Findings were correlated with haemodynamic data in five patients who had undergone cardiac catheterisation studies.
RESULTS
In mild cases of constriction a single wobble of the IVS was seen during normal respiration. In more moderate cases a double motion of the septum (termed "double wobble") was seen where the septum bowed initially into the left ventricle (LV) cavity in diastole then relaxed to the middle only to deviate again into the LV cavity late in diastole after atrial contraction. In severe cases, the septum bowed into the LV cavity for the full duration of diastole (pan-diastolic motion). We describe how inspiration also helped to characterize the severity of constriction especially in mild to moderate cases.
CONCLUSION
Echocardiography appears a simple tool to help diagnose constriction and grade its severity. Larger studies are needed to confirm whether the type of wobble motions helps to grade the severity of constrictive pericarditis.
Keyword
MeSH Terms
Figure
-
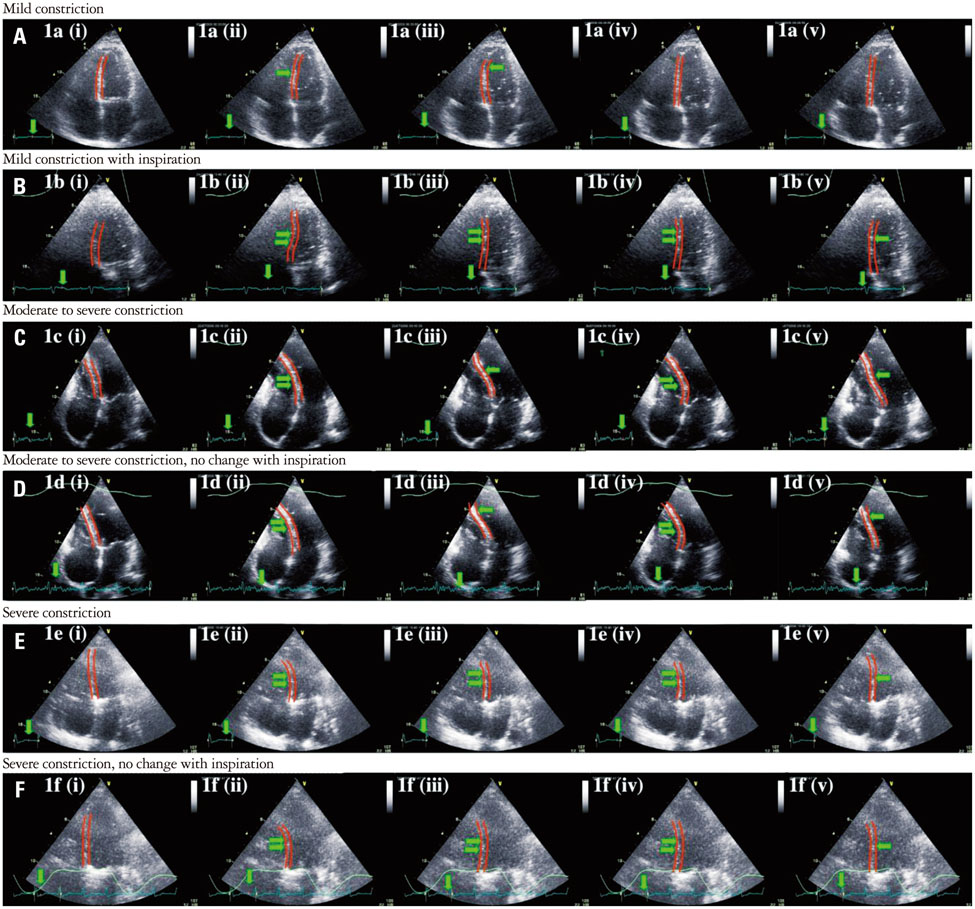
Fig. 1 Mild constriction results in a single wobble of the interventricular septum (A) which is enhanced with inspiration (B). Moderate to severe constriction results in more pronounced motion (C) which is not enhanced by inspiration (D). Severe constriction results in pan-diastolic motion (E) with no change with inspiration (F).
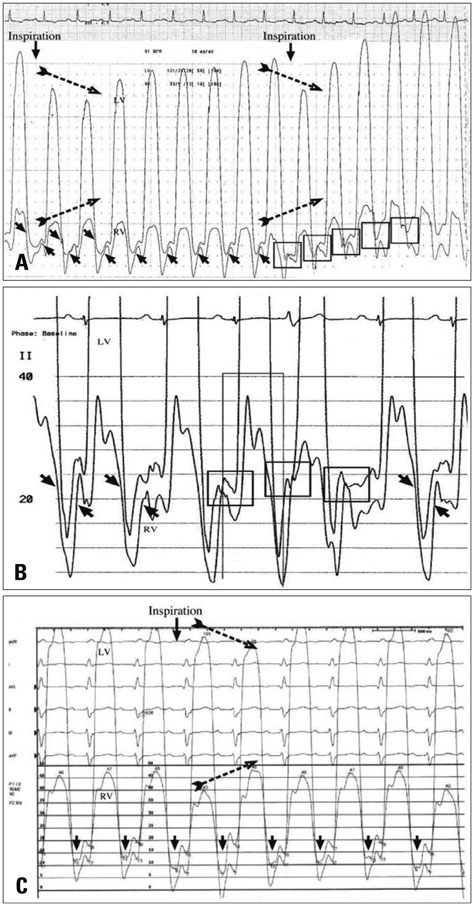
Fig. 2 A: Cardiac catheterisation haemodynamic studies showing near equalisation of diastolic pressures (small arrows) in constrictive pericarditis with divergence of right ventricular (RV) and left ventricular (LV) systolic pressures with inspiration (broken arrows) in patient P2 who had moderate constriction. The first box shows RV greater than LV diastolic pressure after inspiration. B: Near equalisation of diastolic pressures (small arrows) in patient P7 who had moderate to severe constrictive pericarditis after cardiac catheterisation post diuresis. The first box shows RV greater than LV diastolic pressure after atrial contraction and this is probably responsible for the double wobble motion seen before dieresis. C: Diastolic pressures in patient P9 with severe constriction with consistently higher RV compared to LV diastolic pressures (small downward pointing arrows) which explains the pan-diastolic interventricular septum motion seen on echocardiography.
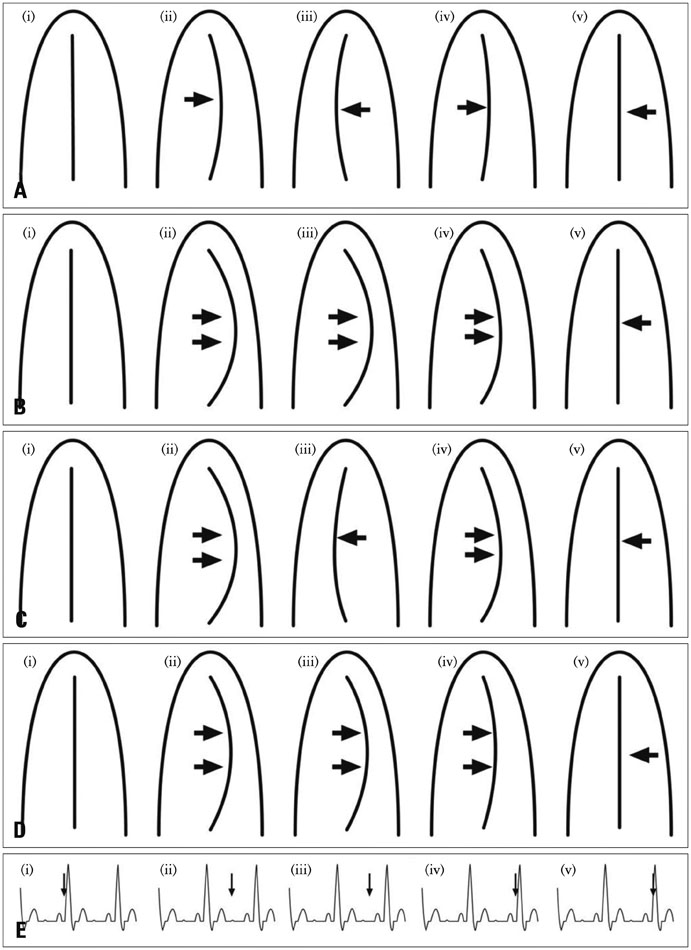
Fig. 3 Schematic diagram showing that the degree of septal deviation caused by constrictive pericarditis, as seen with echocardiography, varies with clinical severity. The figure illustrates the single wobble motion of the septum (indicated by the arrows) in mild constriction (A), and this septal motion is enhanced with inspiration (B). With moderate to severe constriction, the initial septal deviation occurs in early diastole (C (ii)) followed by movement into the right ventricular cavity in mid-diastole (C (iii)). This is then followed by a second incursion into the left ventricular (second or double wobble) after atrial contraction (C (iv)). Unlike mild constriction, inspiration has no effect on interventricular septum movement in patients with moderate to severe constriction (D). Pan-diastolic deviation of the septum without inspiratory enhancement in severe constriction (D). E shows the timing of the septal movements in relation to the electrocardiogram tracing. C (i) and C (v) represent the beginning and end of the cardiac cycle.
Reference
-
1. Candell-Riera J, García del Castillo H, Permanyer-Miralda G, Soler-Soler J. Echocardiographic features of the interventricular septum in chronic constrictive pericarditis. Circulation. 1978; 57:1154–1158.
Article2. Hatle LK, Appleton CP, Popp RL. Differentiation of constrictive pericarditis and restrictive cardiomyopathy by Doppler echocardiography. Circulation. 1989; 79:357–370.
Article3. Himelman RB, Lee E, Schiller NB. Septal bounce, vena cava plethora, and pericardial adhesion: informative two-dimensional echocardiographic signs in the diagnosis of pericardial constriction. J Am Soc Echocardiogr. 1988; 1:333–340.
Article4. Hurrell DG, Nishimura RA, Higano ST, Appleton CP, Danielson GK, Holmes DR Jr, Tajik AJ. Value of dynamic respiratory changes in left and right ventricular pressures for the diagnosis of constrictive pericarditis. Circulation. 1996; 93:2007–2013.
Article5. Talreja DR, Nishimura RA, Oh JK, Holmes DR. Constrictive pericarditis in the modern era: novel criteria for diagnosis in the cardiac catheterization laboratory. J Am Coll Cardiol. 2008; 51:315–319.
Article6. Feneley M, Gavaghan T. Paradoxical and pseudoparadoxical interventricular septal motion in patients with right ventricular volume overload. Circulation. 1986; 74:230–238.
Article7. Giorgi B, Mollet NR, Dymarkowski S, Rademakers FE, Bogaert J. Clinically suspected constrictive pericarditis: MR imaging assessment of ventricular septal motion and configuration in patients and healthy subjects. Radiology. 2003; 228:417–424.
Article8. Francone M, Dymarkowski S, Kalantzi M, Bogaert J. Real-time cine MRI of ventricular septal motion: a novel approach to assess ventricular coupling. J Magn Reson Imaging. 2005; 21:305–309.
Article9. Francone M, Dymarkowski S, Kalantzi M, Rademakers FE, Bogaert J. Assessment of ventricular coupling with real-time cine MRI and its value to differentiate constrictive pericarditis from restrictive cardiomyopathy. Eur Radiol. 2006; 16:944–951.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Clinical Course of Tuberculous Pericarditis in Immunocompetent Hosts Based on Serial Echocardiography
- Echocardiographic Evaluation of Constrictive Pericarditis
- Constrictive Pericarditis Following Acute Idiopathic Pericarditis
- Pericardiectomy by a Left Limited Anterolateral Thoracotomy for Constrictive Pericarditis after Cardiac Surgery: 2 case reports
- The Cardiac MR Images and Causes of Paradoxical Septal Motion
