Emergency In Situ Bypass during Middle Cerebral Artery Aneurysm Surgery: Middle Cerebral Artery-Superficial Temporal Artery Interposition Graft-Middle Cerebral Artery Anastomosis
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Neurosurgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. bang78425@hanmail.net
- KMID: 2066929
- DOI: http://doi.org/10.3340/jkns.2012.51.5.292
Abstract
- Many reports have been published on complications related to middle cerebral artery (MCA) aneurysm surgical clipping procedures. We report an emergency intracranial in situ bypass surgery case which was performed as a rescue procedure after aneurysmal neck laceration during clipping of an MCA large aneurysm. In this case, we performed in situ M3-superficial temporal artery (STA) interposition graft-M3 bypass procedure. If a STA-MCA anastomosis is not available under MCA flow obstruction, we can consider an emergency in situ MCA-MCA bypass procedure with or without an STA interposition graft.
MeSH Terms
Figure
-

Fig. 1 The sizes of the aneurysms were measured by transfemoral carotid angiography. A and B: Middle cerebral artery bifurcation aneurysm (11.3×9.0 mm). C: A2-3 aneurysm (7.1×3.1 mm).
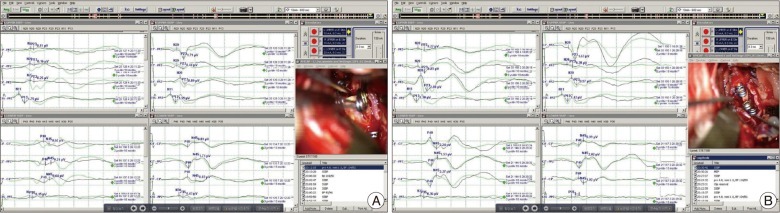
Fig. 2 Intraoperative evoked potential changes. After re-clipping of the middle cerebral artery aneurysm, SSEP (A) show a decreased amplitude near a flat wave (duration=55 minutes). After the M2-STA-M2 bypass procedure, recovered wave patterns are found in SSEP (B). SSEP: somatosensory evoked potential, STA: superficial temporal artery.
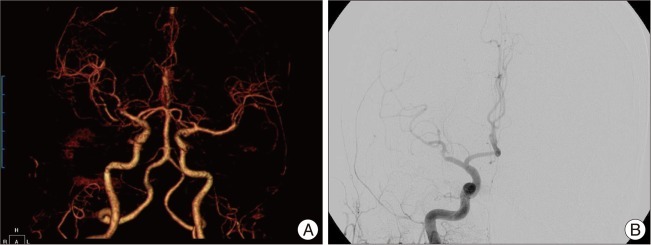
Fig. 3 A: Immediate postoperative computed tomography angiography demonstrates good M2 trunk flow of with good patency of the bypass graft. B: Emergency TFCA demonstrates occlusion of the inferior M2 trunk, and no visible bypass pedicle is detected. TFCA: transfemoral carotid angiography.
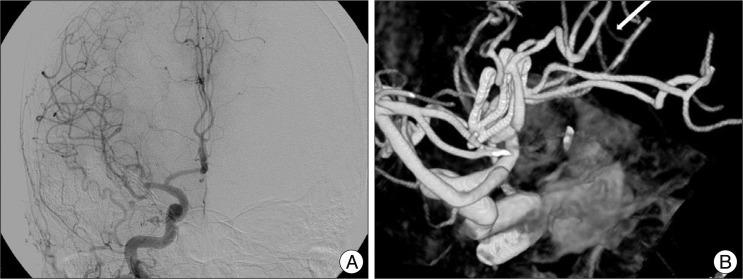
Fig. 4 Follow-up TFCA at postoperative two weeks reveals complete recanalization of the M2 inferior trunk (A) with intact STA interposition graft (B, white arrow). STA: superficial temporal artery, TFCA: transfemoral carotid angiography.
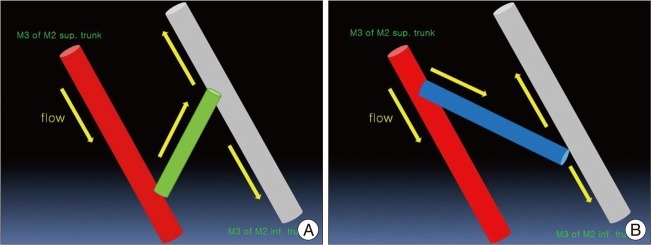
Fig. 5 The mimetic diagram of M3-STA-M3 anastomosis. A: In this case, we performed an anastomosis with an acute angle between the M3 of superior M2 trunk and the STA graft with an obtuse angle between the STA graft and the M3 of M2 inferior trunk. So, the flow direction is not "natural," and the flow burden of the M2 superior trunk might have increased. B: We believe that ideal and natural M3-STA-M3 anastomosis should be as diagrammed, with the natural flow direction from the M3 of superior M2 trunk toward the STA interposition graft with an obtuse angle. STA: superficial temporal artery.
Reference
-
1. Ahn JS, Kwun BD. Complications in middle cerebral artery aneurysm surgery. J Korean Neurosurg Soc. 1998; 27:1762–1768.2. Bederson JB, Spetzler RF. Anastomosis of the anterior temporal artery to a secondary trunk of the middle cerebral artery for treatment of a giant M1 segment aneurysm. Case report. J Neurosurg. 1992; 76:863–866. PMID: 1564547.
Article3. Dashti R, Hernesniemi J, Niemelä M, Rinne J, Porras M, Lehecka M, et al. Microneurosurgical management of middle cerebral artery bifurcation aneurysms. Surg Neurol. 2007; 67:441–456. PMID: 17445599.
Article4. Karhunen PJ. Neurosurgical vascular complications associated with aneurysm clips evaluated by postmortem angiography. Forensic Sci Int. 1991; 51:13–22. PMID: 1752589.
Article5. Lanzino G, Spetzler RF. Clip wrapping for partial avulsion of the aneurysm neck. Technical note. J Neurosurg. 2003; 99:931–932. PMID: 14609177.6. Quiñones-Hinojosa A, Lawton MT. In situ bypass in the management of complex intracranial aneurysms: technique application in 13 patients. Neurosurgery. 2005; 57:140–145. PMID: 15987580.
Article7. Sanai N, Zador Z, Lawton MT. Bypass surgery for complex brain aneurysms: an assessment of intracranial-intracranial bypass. Neurosurgery. 2009; 65:670–683. discussion 683. PMID: 19834371.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Middle Cerebral Artery AneurysmOriginating Near the Site of Anastomosis after Superficial Temporal Artery-Middle Cerebral Artery Bypass: Case Report
- Duplication of the Middle Cerebral Artery: Case Report
- Middle Cerebral Artery Variations Associated with Intracranial Aneurysmal Rupture
- Giant Serpentine Aneurysm of the Middle Cerebral Artery
- Distal Middle Cerebral Artery M4 Aneurysm Surgery Using Navigation-CT Angiography
