Staged Management of High Energy Proximal Tibia Fractures with Severe Soft Tissue Damage
- Affiliations
-
- 1Department of Orthopaedic Surgery, Chungnam National University School of Medicine, Daejeon, Korea. osdr69@cnu.ac.kr
- 2Department of Plastic and Reconstructive Surgery, Chungnam National University School of Medicine, Daejeon, Korea.
- KMID: 2063903
- DOI: http://doi.org/10.12671/jkfs.2009.22.3.152
Abstract
-
PURPOSE: To find out the efficiency of two staged operation of patients with high energy proximal tibia fracture with severe soft tissue damage, the first step being external fixation, and the second, internal fixation with plates.
MATERIALS AND METHODS
The study group was the 42 patients who had followed for one year out of a group of 56, performed the first step external fixation and the second step internal fixation with plates retrospectively, from March 2003 to March 2007. The average age of the study group was 51.4, 26 men, and 16 women participating in this study. The average time of follow up was 32 months. In the final follow up, investigations of the radiological assessments and functional abilities of the bony fusion were carried out along with the complications of the soft tissue.
RESULTS
The duration after the first step external fixation until second step internal fixation to be performed was 14.9 (6~40) days in average. The final bone fusion took about 15 weeks, and according to the final follow up, the range of motion of the knee was around 110.8 degrees (6.2~117 degrees). In 31 cases, only the internal fixation was performed, while in 11 cases, soft tissue reconstruction was carried out with the internal fixations. As for the complications there were 2 cases of deep soft tissue infection, 2 cases of nonunion, 1 case of malunion and 1 case of knee joint stiffness.
CONCLUSION
In cases of proximal tibia fracture with severe soft tissue damage, external fixation was important to secure the safety of the fracture, carry forward the anatomical alignment, plan the soft tissue safety and manage the wound to decrease the number of microbial in the next operation, which is the internal fixation with plates.
Keyword
MeSH Terms
Figure
-

Fig. 1 53 year-old man with a proximal tibia fracture (AO/OTA type C2) by a pedestrian traffic accident. (A, B) Preoperative anteroposterior and lateral radiographs showing the comminution and the lateral condylar depression, (C) and the swelling of knee joint and surrounding soft tissues were severe. (D, E) External fixation was performed after the day of accident, and these postoperative radiographs shows well aligned fracture fragments. (F, G) Internal fixation was performed after 17 days, and these radiographs shows firm fixation with a lateral periarticular plate and additional K-wire fixation to preserve the articular line of the knee.

Fig. 2 45 year-old man with a proximal tibia fracture (AO/OTA type C3, open GIIIb) by a motorcycle traffic accident. Preoperative anteroposterior and lateral radiographs showing the splitting of the tibial condyle and severe comminuted, displaced fragments. (A, B) The soft tissue defect was about 25×10 cm as shown, (C, D) and after copious irrigation and wide marginal debridement was performed at operation room, external fixation was performed immediately. (E, F) Internal fixation was performed after 9 days, and anterolateral thigh free flap was performed by plastic surgeons concurrently. (G, H) The radiographs shows fixation with lateral periarticular plate medial locking compression plate and relatively preserved articular surface of the knee.

Fig. 3 The 12 months follow up (A) anteroposterior and (B) lateral radiographs of the patient described in Fig. 1. The articular surface was congruent and union was achieved successfully. The range of motion was 5 to 120 degree, and patient had mild pain on knee when forceful flexion and extension was performed.
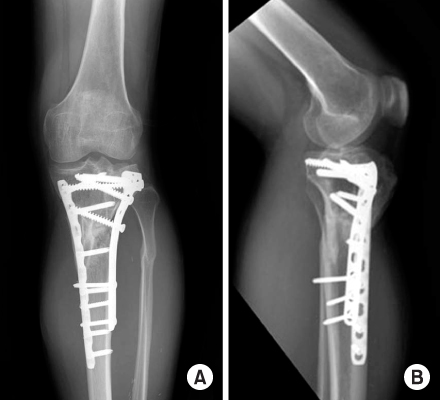
Fig. 4 The 30 months follow up (A) anteroposterior and (B) lateral radiographs of the patient described in Fig. 2. The articular surface was congruent and union was achieved successfully. The range of motion was 0 to 130 degrees, but the patient suffered in pain when full weight bearing was performed.
Reference
-
1. Anglen JO, Healey WV. Tibial plateau fractures. Orthopedics. 1988; 11:1527–1534.
Article2. Blokker CP, Rorabeck CH, Bourne RB. Tibial plateau fractures. An analysis of the results of treatment in 60 patients. Clin Orthop. 1984; 182:193–199.
Article3. Delamarter RB, Hohl M, Hopp E Jr. Ligament injuries associated with tibial plateau fractures. Clin Orthop Relat Res. 1990; 250:226–233.
Article4. Egol KA, Tejwani NC, Capla EL, Wolinsky PL, Koval KJ. Staged management of High-energy proximal tibia fracture (OTA types 41): the results of a prospective, standardized protocol. J Orthop Trauma. 2005; 19:448–455.5. Fernandez DL. Anterior approach to the knee with osteotomy of the tibial tubercle for bicondylar tibial fractures. J Bone joint Surg Am. 1988; 70:208–219.
Article6. Giannoudis PV. Surgical priorities in damage control in polytrauma. J Bone Joint Surg Br. 2003; 85:478–483.
Article7. Gottschalk FAB, Graham AJ, Morein G. The management of severely comminuted fractures of the femoral shaft, using the external fixator. Injury. 1985; 16:377–381.
Article8. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones. Retrospective and prospective analysis. J Bone Joint Surg. 1976; 58:453–458.
Article9. Haidukewych GJ, Collinge CA. Conversion of temporary external fixation to formal internal fixation for complex for complex periarticular injuries of the lower extremity: is there an infection risk? In : Presented at the American academy of orthopaedic surgeons annual meeting; Dallas, Texas: 2002.10. Mallik AR, Covall DJ, Whitelaw GP. Internal versus external fixation of bicondylar tibial plateau fracture. Orthop Rev. 1992; 21:1433–1436.11. Mikulak SA, Gold SM, Zinar DM. Small wire external fixation of high energy tibial plateau fractures. Clin Orthop Relat Res. 1998; 356:230–238.
Article12. Mills WJ, Nork SE. Open reduction and internal fixation of high-energy tibial plateau fractures. Orthop Clin North Am. 2002; 33:177–198.
Article13. Moore TM, Patzakis MJ, Harvey JP. Tibial plateau fractures: definition, demographics, treatment rationale, and long-term results of closed traction management or operative reduction. J Orthop Trauma. 1987; 1:97–119.14. Nowotarski PJ, Turen CH, Brumback RJ, Scarboro JM. Conversion of external fixation to intramedullary nailing for the shaft of the femur in multiply injured patients. J Bone joint Surg. 2000; 82:781–788.
Article15. Park TW, Cho SD, Cho YS, Kim BS, Lew S, Hwang SY. Treatment of proximal tibia fracture with hybrid external fixator. J Korean Soc Fract. 2001; 14:285–290.
Article16. Patterson MJ, Cole JD. Two staged delayed open reduction and internal fixation of severe pilon fractures. J Orthop Trauma. 1999; 13:85–91.
Article17. Perry CR, Evans LG, Rice S, Fogarfy J, Burdge RE. A new surgical approach to fractures of the lateral tibial plateau. J Bone Joint Surg Am. 1984; 66:1236–1240.
Article18. Rasmussen PS. Tibial condylar fractures. Impairment of knee joint stability as an indication for surgical treatment. J Bone Joint Surg Am. 1973; 55:1331–1350.19. Remiger AR, Miclau T, Neuer W. A simple technique for creating hybrid fixators using a modified AO single adjustable clamp. J Orthop Trauma. 1997; 11:54–56.
Article20. Scalea TM, Boswell AS, Scott JD, Mitchell KA, Kramer ME, Pollak AN. External fixation as a bridge to intramedullary nailing for patients with multiple Injuries and with femur fractures:damage control orthopaedics. J Trauma. 2000; 48:613–623.
Article21. Schatzker J, McBroom R, Bruce D. The tibial plateau fractures. The Toronto experience 1968-1975. Clin Orthop Relat Res. 1979; 138:94–104.22. Sirkin M, Sanders R, Di Pasquale T, Herscovici Jr. A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma. 1999; 13:78–84.
Article23. Stamer DT, Schenk R, Staggers B, Aurori K, Aurori B, Behrens FF. Bicondylar tibial plateau fractures treated with a hybrid ring external fixator: a preliminary study. J Orthop Trauma. 1994; 8:455–461.
Article24. Tornetta P 3rd, Weiner L, Bergman M, et al. Pilon fracture: treatment with combined internal and external fixation. J Orthop Trauma. 1993; 7:489–496.25. Watson JT. High-energy fractures of the tibial plateau. Orthop Clin North Am. 1994; 25:723–752.
Article26. Watson JT, Coufal C. Treatment of complex lateral plateau fractures using Ilizarov techniques. Clin Orthop Relat Res. 1998; 353:97–106.
Article27. Weiner LS, Kelly M, Yang E, et al. The use of combination internal fixation and hybrid external fixation in severe proximal fractures. J Orthop Trauma. 1995; 9:244–250.28. Waddell JP, Johnston DWC, Neidre A. Fractures of the tibial plateau: a review of ninety-five patients and comparison of treatment methods. J Trauma. 1981; 21:376–381.
Article29. Young MJ, Barrack RL. Complications of internal fixation of tibial plateau fractures. Orthop Rev. 1994; 23:149–154.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Distal Tibia Fractures
- Acute Shortening and Gradual Lengthening for a Comminuted Tibia Fracture with Massive Bone and Soft Tissue Defect: Case Report
- Result of Staged Operation in Ruedi-Allgower Type II and III Open Tibia Pilon Fractures with Severe Comminution
- Treatment of High-energy Distal Tibia Intraarticular Fractures with Two-staged Delayed Minimal Invasive Plate Osteosynthesis
- The Problems of Locked Intramedullary Nailing in the Proximal Shaft Fractures of the Tibia
