Compressive Partial Neuropathy of Axillary Nerve Resulting from Antero-Inferior Paralabral Cyst in an Adolescent Overhead Athlete
- Affiliations
-
- 1Center for Shoulder, Elbow and Sports at Neon Orthopedic Clinic, Seoul, Korea.
- 2Department of Orthopedic Surgery, Seoul Red-Cross Hospital, Seoul, Korea. remindh@naver.com
- 3Department of Orthopedic Surgery, Konkuk University School of Medicine, Seoul, Korea.
- 4Department of Orthopedic Surgery, Inje University Haeundae Paik Hospital, Busan, Korea.
- KMID: 2054039
- DOI: http://doi.org/10.5763/kjsm.2015.33.1.34
Abstract
- Paralabral cysts of the shoulder are rare, and there are few reports available that describe anteroinferior paralabral cysts arising from a detached antero-inferior glenoid labral tear without shoulder instability. We report an antero-inferior labral tear without shoulder instability in adolescent overhead athlete associated with paralabral cyst that leads to axillary nerve neurapraxia. Although nonoperative management of such labral lesions may provide symptoms of relief, it may not be enough for the athlete to return to the game. However, surgical treatment in this case provides successful recovery and rapid return to playing baseball play without having to worry about the progression of muscle denervation.
Keyword
Figure
-
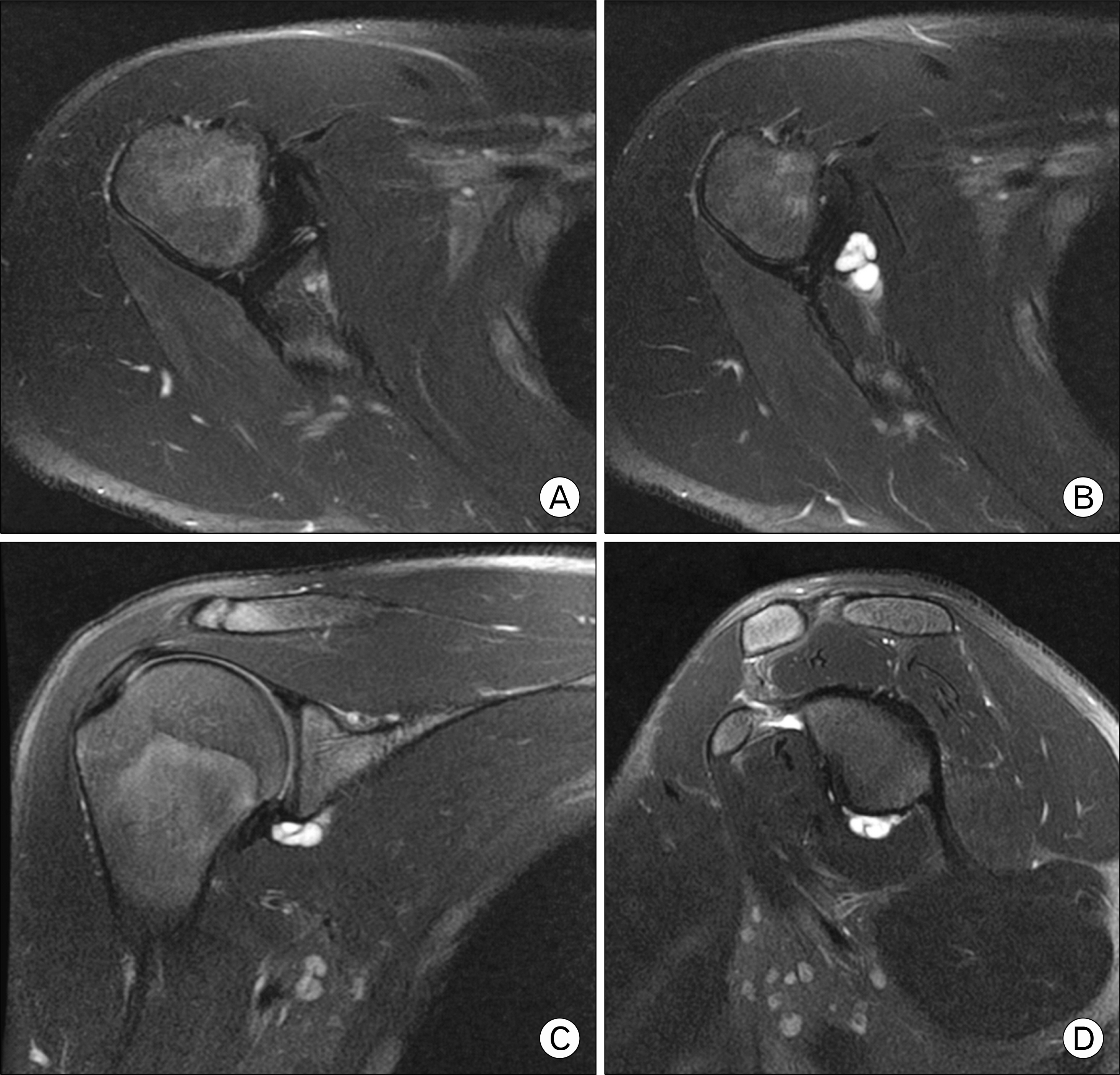
Fig. 1. Axial T2-weighted fat-suppressed (A, B), coronal T2-weighted fat-suppressed (C) and sagittal T2-weighted fat-suppressed (D) magnetic resonance images of the right shoulder. They are demonstrating an antero-inferior labral tear (from the 4-o’clock to 5-o’clock position) with adjacent 13 mm×15 mm×12 mm multiloculated paralabral cyst (from the 5-o’clock to 6-o’clock position) not extending into the quadrilateral space.

Fig. 2. Coronal T2-weighted fat-suppressed (A) and sagittal T2-weighted fat-suppressed (B) magnetic resonance images of the right shoulder. Where denervation edema or teres minor mild atrophy was appreciated due to mild increased signal intensity (white arrows).

Fig. 3. Arthroscopic view of the right shoulder with use of the superior portal (lateral decubitus position). (A) Arthroscopic findings showed that the antero-inferior capsule-labral complex had partial detachment (from the 4-o’clock to 6-o’clock position) from the glenoid. (B) The cyst and its multiloculated subcompartments were thoroughly decompressed under direct vision with blunt instruments and a shaver device. Then the anteroposterior margin of the glenoid was freshened and decorticated with the use of a shaver device. (C) Anatomic arthroscopic repair of the antero-inferior labral complex to the glenoid margin was performed with the use of two Bio Mini-Revo suture anchors (ConMed Linvatec, Largo, FL, USA) with one placed at the 4:30-clock position and one placed at the 5:30-clock position. A simple suture configuration was utilized.
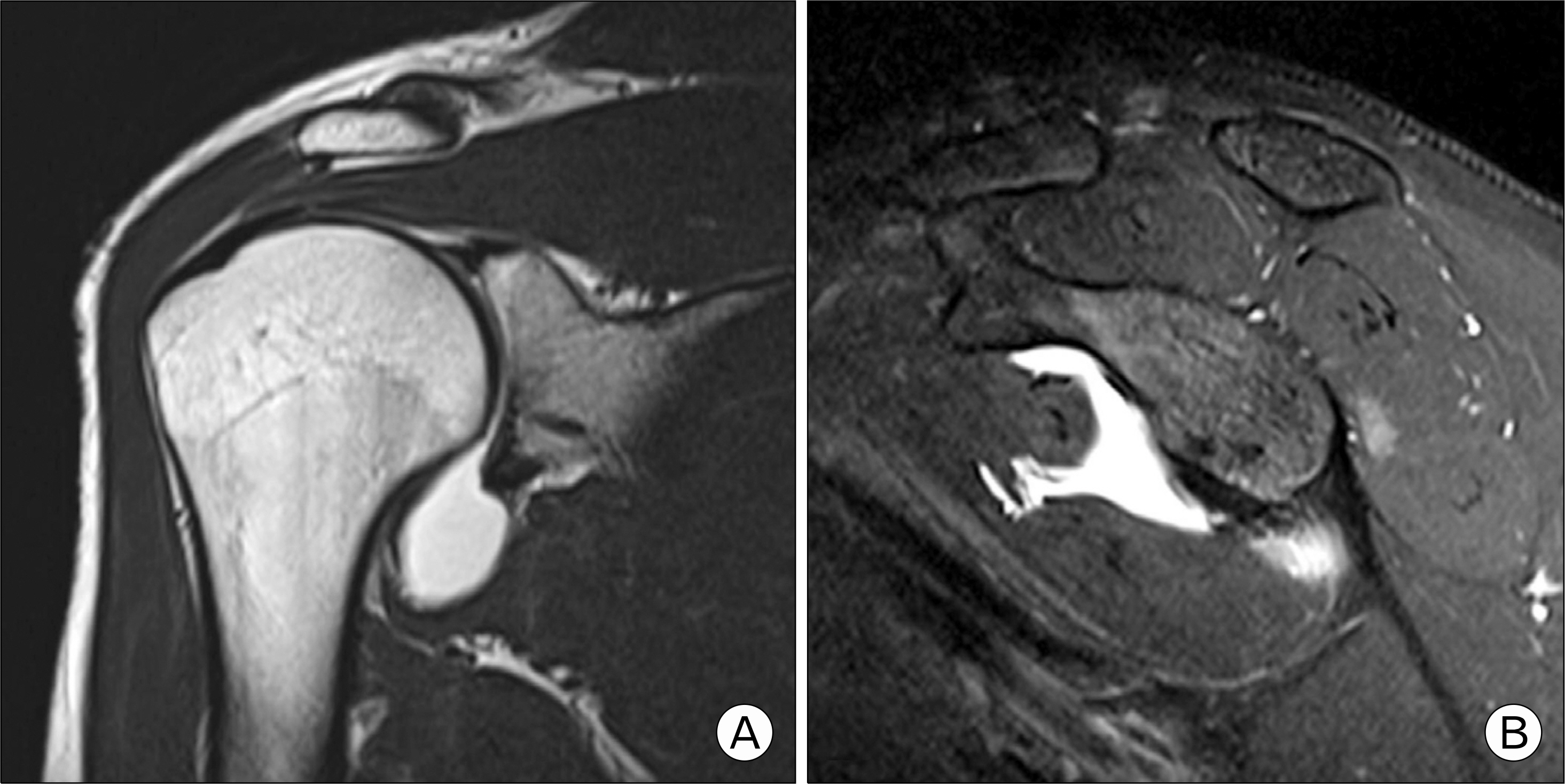
Fig. 4. (A, B) The twelve-month follow-up MRA (magnetic resonance arthrography) showed complete resolution of the paralabral cyst.
Cited by 1 articles
-
Osseous Erosion by Spinoglenoid Ganglion Cyst in Adolescent Baseball Player: A Case Report
Hong Ki Jin, Hyung Lae Cho, Ji Hoon Kim
Korean J Sports Med. 2021;39(4):188-192. doi: 10.5763/kjsm.2021.39.4.188.
Reference
-
1.Li X., Ma R., Nielsen NM., Gulotta LV., Dines JS., Owens BD. Management of shoulder instability in the skeletally immature patient. J Am Acad Orthop Surg. 2013. 21:529–37.
Article2.Dietz SO., Lichtenberg S., Habermeyer P. Non-traumatic shoulder instability in an athletic patient with a periglenoidal cyst and a glenoid labral tear. Acta Orthop Belg. 2003. 69:373–6.3.Lee BC., Yegappan M., Thiagarajan P. Suprascapular nerve neuropathy secondary to spinoglenoid notch ganglion cyst: case reports and review of literature. Ann Acad Med Singapore. 2007. 36:1032–5.4.Schroder CP., Skare O., Stiris M., Gjengedal E., Uppheim G., Brox JI. Treatment of labral tears with associated spinoglenoid cysts without cyst decompression. J Bone Joint Surg Am. 2008. 90:523–30.
Article5.Gartsman GM. Shoulder arthroscopy. 2nd ed.Philadelphia: Saunders/Elsevier;2009.6.Ferrick MR., Marzo JM. Ganglion cyst of the shoulder associated with a glenoid labral tear and symptomatic glenohumeral instability: a case report. Am J Sports Med. 1997. 25:717–9.7.Yukata K., Imada K., Yoshizumi Y., Tamano K., Hosokawa S., Nakaima N. Intra-articular ganglion cyst (paralabral cyst) of the shoulder associated with recurrent anterior dislocation: a case report. J Shoulder Elbow Surg. 2002. 11:95–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Can Suprascapular Venous Engorgement with a Paralabral Cyst in the Shoulder Aid the Diagnosis of Suprascapular Neuropathy?: A Cohort Study of Level of Evidence III
- Acetabular Paralabral Cyst as a Rare Cause of Obturator Neuropathy: A Case Report
- Multidirectional Instability Accompanying an Inferior Labral Cyst
- Arthroscopic Decompression of an Inferior Paralabral Cyst of the Shoulder in an Elderly Patient: A Case Report
- Cubital Tunnel Syndrome by Anconeus Epitrochlearis in an Adolescent
