Electrolyte Blood Press.
2006 Mar;4(1):47-52. 10.5049/EBP.2006.4.1.47.
Pathogenesis and Treatment of Dyskalemia in Maintenance Hemodialysis and CAPD
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Hanyang University, Guri, Korea. kimhj@hanyang.ac.kr
- KMID: 2052269
- DOI: http://doi.org/10.5049/EBP.2006.4.1.47
Abstract
- In end-stage renal disease (ESRD) patients regardless of dialysis modes, i.e. maintenance hemodialysis (HD) and continuous ambulatory peritoneal dialysis (CAPD), potassium (K) homeostasis is regulated primarily via dialysis and extrarenal K regulation in the diverse daily K intake. However, K metabolism has been known to differ greatly between the two main methods of dialysis. Hyperkalemia is a common complication (10-24%) and the most common cause of the death (3-5%) among electrolyte disorders in patients on maintenance HD. On the contrary, hypokalemia (10-36%) is responsible for a rather common complication and independent prognostic factor on CAPD. Although excessive K intake or inadequate dialysis on maintenance HD and poor nutritional K intake on CAPD are accused without doubts upto 50% of ESRD patients as a primary cause of the K-imbalance, i.e. hyperkalemia on HD and hypokalemia on CAPD, other contributory factors including certain medications and unknown causes remain still to be resolved. Accordingly, the effects of medications as another source of K-imbalance on HD with RAS blockades and beta blockers as well as those of conventional and glucose-free dialysates (Icodextrin) for internal K-redistribution on CAPD were evaluated with reviewing the literatures and our data. Furthermore, new developments in the clinical managements of hyperkalemia on HD following the exclusion of pseudohyperkalemia before the initiation of dialysis were suggested, especially, by the comparison of the effects between mono- and dual-therapy with medications for transcellular K shifting in the emergent situation. Also, the intraperitoneal K administration via conventional glucose-containing (2.5%) and glucose-free dialysates (Icodextrin) as a specific route of K-supplementation for hypokalemia on CAPD was examined for its efficiency and the degree of intracellular K shift between these two different types of dialysates.
MeSH Terms
Figure
-
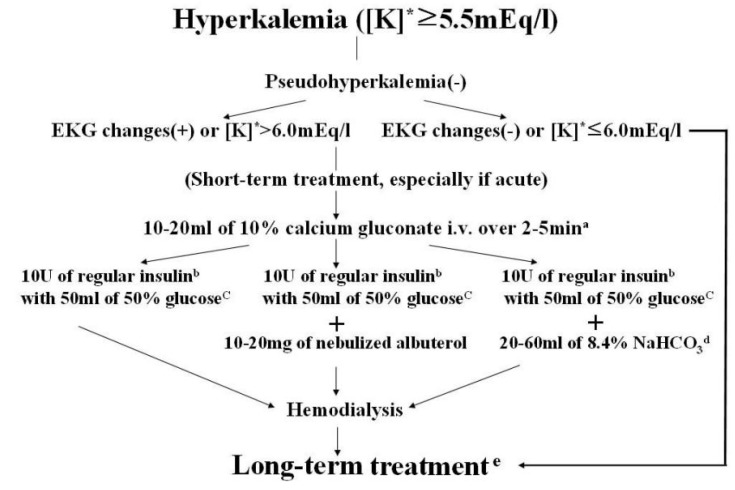
Fig. 1 Flow chart for treatment of hyperkalemia. [K]* : serum potassium concentration. a : Can be repeated until resolving EKG changes. b : Intravenous bolus injection. c : If blood glucose is more than 250 mg/dL, can be omitted. d : Not proven unanimously. e : See this paper for instructions (Kim HJ, Han SW. Therapeutic approach to hyperkalemia, Nephron 92(suppl 1):33-40, 2002).
Cited by 1 articles
-
Potassium Balances in Maintenance Hemodialysis
Hoon Young Choi, Sung Kyu Ha
Electrolyte Blood Press. 2013;11(1):9-16. doi: 10.5049/EBP.2013.11.1.9.
Reference
-
1. Sherman RA, Hwang ER, Bernholc AS, Eisinger RP. Variability in potassium removal by hemodialysis. Am J Nephrol. 1986; 6:284–288. PMID: 3777037.
Article2. Szeto CC, Chow KA, Kwan BCH, Leung CB, Chung KY, Law MC, Kam-Tao . Hypokalemia in Chinese peritoneal dialysis patients: Prevalence and prognostic implication. Am J Kidney Dis. 2005; 46:128–135. PMID: 15983966.
Article3. Amici G, Orrasch M, Rin GD, Bocci C. Hyperinsulinism reduction associated with icodextrin treatment in continuous ambulatory peritoneal dialysis patients. Adv Perit Dial. 2001; 17:81–85.4. Bastl C, Hayslett JP, Binder HJ. Increased large intestinal secretion of potassium in renal insufficiency. Kidney Int. 1977; 12:9–16. PMID: 142857.
Article5. Weiner D, Wingo CS. Hyperkalemia: a potential silent killer. J Am Soc Nephrol. 1998; 9:1535–1545. PMID: 9697678.
Article6. Kim JH, Kahng KW, Kim JH, Kim HJ, Park CH, Kang CM, Park HC. The survival rate and causes of death in patients with chronic renal failure on hemodialysis. Korean J Med. 1993; 44:294–300.7. Cho HD, Choi CR, Choi SI, Kang TY, Lee DK, Ryu JH, Han SW, Kim HJ. The Analysis of Causes and Treatments of Hyperkalemia. Korean J Nephrol. 2001; 20:882–889.8. Castellino P, Bia MJ, DeFronzo RA. Adrenergic modulation of potassium metabolism in uremia. Kidney Int. 1990; 37:793–798. PMID: 2308263.
Article9. Nowicki M, Miszczak-Kuban J. Nonselective beta-adrenergic blockade augments fasting hyperkalemia in hemodialysis patients. Nephron. 2002; 91:222–227. PMID: 12053057.
Article10. Lee JU, Lee OY, Yang SC, Han DS, Sohn JH, Kim SK, Kim HJ, Koh HK, Jung JH, Nam SW, Paik IK, Lee CB. The influence of nonselective beta-adrenergic blockade (carteolol) and ACE inhibitor (captopril) in plasma potassium on maintenance hemodialysis. Korean J Med. 1997; 52:149–155.11. Knoll GA, Sahgal A, Nair RC, Graham J, Van Walraven C, Burns KD. Renin-angiotensin system blockade and the risk of hyperkalemia in chronic hemodialysis patients. Am J Med. 2001; 112:110–114. PMID: 11835948.
Article12. Hussain S, Dreyfus DE, Marcus RJ, Biederman RWW, McGill RL. Is spironolactone safe for dialysis patients? Nephrol Dial Transplant. 2003; 18:2364–2368. PMID: 14551367.
Article13. Han SW, Won YW, Kim HJ. No impact of hyperkalemia with renin-angiotensin system blockades in maintenance hemodialysis patients [Abstract]. (Submitted to NDT 2006).14. Blumberg A, Weidman P, Ferrari P. Effect of prolonged bicarbonate administration on plasma potassium in terminal renal failure. Kidney Int. 1992; 41:369–374. PMID: 1552710.
Article15. Kim HJ. The combined effect of bicarbonate and insulin with glucose in acute therapy of hyperkalemia in end-stage renal disease patients. Nephron. 1996; 38:869–872.16. Kim HJ. Acute therapy with the combined regimen of bicarbonate and beta-2 agonist (salbutamol) in chronic renal failure patients. J Korean Med Sci. 1997; 12:111–116. PMID: 9170015.17. Allon M, Copkney C. Albuterol and insulin for treatment of hyperkalemia in hemodialysis patients. Kidney Int. 1990; 38:869–872. PMID: 2266671.
Article18. Choi CR, Cho HD, Kang TY, Lee JS, Han H, Jung CI, Lee DK, Ryu JH, Han SW, Kim HJ. Pseudohyperkalemia on Maintenance Hemodialysis. Korean J Nephrol. 2001; 20:842–850.19. Kim HJ, Han SW. Therapeutic approach to hyperkalemia. Nephron. 2002; 92(suppl 1):33–40. PMID: 12401936.
Article20. Mathialahan T, Sandle GI. Dietary potassium and laxatives as regulators of colonic potassium secretion in end-stage renal disease. Nephrol Dial Transplant. 2003; 18:341–347. PMID: 12543890.21. Furuya R, Kumagai H, Sakao T, Maruyama Y, Hishida A. Potassium-lowering effect of mineralocorticoid therapy in patients undergoing hemodialysis. Nephron. 2002; 92:576–581. PMID: 12372940.
Article22. Serra A, Uehlinger DE, Ferrari P, Dick B, Frey BM, Frey FJ, Vogt B. Glycyrrhetinic acid decreases plasma potassium concentrations in patients with anuria. J Am Soc Nephrol. 2002; 13:191–196. PMID: 11752037.
Article23. Kim HJ, Han SW, Choi HY, Lee HY. Comparison of serum potassium (K) profile between the conventional glucose solution and icodextrin in CAPD [Abstract]. (submitted to ERA-EDTA 2006).24. Kim HJ, Kim JY, Son BK, Lee KW. High prevalence of hypokalemia associated with underlying malnutrition and sustained dialysate K loss in CAPD patients on admission [Abstract]. J Am Soc Nephrol. 1999; 10:317.25. Tziviskou E, Musso C, Bellizzi V, Khandelwal M, Wang T, Savaj S, Oreopoulos DG. Prevalence and pathogenesis of hypokalemia in patients on chronic peritoneal dialysis: One center's experience and review of the literature. Int Urol Nephrol. 2003; 35:429–434. PMID: 15160552.
Article26. Kim HJ, Park IG. Acute potassium repletion by intraperitoneal administration in hypokalemic CAPD patients [Abstract]. ERA-EDTA. 1997; 266A.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Potassium Balances in Maintenance Hemodialysis
- Serum Glycosylated Albumin and Fructosamine in Patients with Chronic Renal Failure Undergoing Dialysis
- Effects of CAPD on Cardiac Function in Patients with End-Stage Renal Disease: in Comparison with Hemodialysis
- A case of diabetic hyperosmolar coma treated successfully with conversion to hemodialysis in a chronic renal failure patient on CAPD treatment
- A case of sclerosing encapsulating peritonitis presenting a huge pseudocyst formation in end stage renal failure on the maintenance hemodialysis
