The Clinical Meaning of Benign Colon Uptake in 18F-FDG PET: Comparison with Colonoscopic Findings
- Affiliations
-
- 1Department of Internal Medicine, Ewha Medical Reseach Institute and Ewha Womans University School of Medicine, Seoul, Korea. jassa@ewha.ac.kr
- 2Department of Nuclear Medicine, Ewha Medical Reseach Institute and Ewha Womans University School of Medicine, Seoul, Korea.
- KMID: 2048852
- DOI: http://doi.org/10.5946/ce.2012.45.2.145
Abstract
- BACKGROUND/AIMS
Benign colon 18F-fluorodeoxyglucose (FDG) uptake is frequently observed in asymptomatic individuals. Aims of this study were to investigate the benign colon uptake by whole body FDG-positron emission tomography (PET) in asymptomatic adults and to correlate those results with colonoscopic and histologic findings.
METHODS
Among 3,540 subjects who had undergone FDG-PET, 43 subjects who were diagnosed to have benign colon uptake in FDG-PET and underwent colonoscopy were retrospectively reviewed. Subjects were classified as diffuse or focal groups based on their FDG uptake patterns. PET results were analyzed together with colonoscopic and histologic findings.
RESULTS
Forty-three subjects showed benign colon uptake in FDG-PET; 28 of them were shown as the diffuse group, while other 15 subjects were classified as the focal group. Five subjects among those showed diffuse uptake were diagnosed as adenoma. Seven among 15 subjects who showed focal uptake were diagnosed as adenocarcinoma (n=2), adenoma (n=3), or non-neoplastic polyp (n=2). Positive predictive values were 25% in the diffuse group and 47% in the focal group.
CONCLUSIONS
We recommend that patients showing benign FDG uptake in the colon should be further evaluated by colonoscopy, especially for patients with focal FDG uptake.
MeSH Terms
Figure
-

Fig. 1 Classification according to benign colon uptake pattern in fluorodeoxyglucose positron emission tomography. (A) Diffuse group. It showed diffuse colon uptake. (B) Focal group. It showed focal colon uptake.
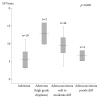
Fig. 2 Per-lesion standardized uptake value intensity (maximum standardized uptake value [SUVmax]) mean and standard deviation for different colonoscopic findings. The neoplastic lesion had significantly increased maximal SUV value (p=0.009) and high grade dysplasia had greater maximal SUV value among adenomas (p=0.02). The SUVmax is 6.1±3.2 for low grade dysplasia adenoma (n=10), 12.9±4.2 for high grade dysplasia adenoma (n=2), 9.6±3.4 for well to moderately differentiated adenocarcinoma (n=44) and 6.6±2.0 for poorly differentiated adenocarcinoma (n=4).

Fig. 3 A 62-year-old male with prostate cancer. (A) Intense focal standardized uptake (maximum standardized uptake value, 4.2) is located in descending colon. (B) A 13-mm polyp is found in colonoscopy. (C) The pathologic diagnosis is villotubular adenoma with focal adenocarcinoma involving mucosa (left, H&E stain, ×40; right, ×200).

Fig. 4 A 70-year-old male with nasopharyngeal cancer. (A) Intense focal standardized uptake (maximum standardized uptake value, 10.1) is located in transverse colon. (B) A 15-mm polyp is found in colonoscopy. (C) The pathologic diagnosis is focal well differentiated adenocarcinoma with coexisting villotubular adenoma (left, H&E stain, ×40; right, ×200).
Reference
-
1. National Cancer Information Center. [Internet]. c2011. cited 2011 Dec 20. Goyang: National Cancer Information Center;Available from: http://www.cancer.go.kr/ncic/cics_f/02/022/index.html.2. Kantorová I, Lipská L, Bêlohlávek O, Visokai V, Trubaĉ M, Schneiderová M. Routine (18)F-FDG PET preoperative staging of colorectal cancer: comparison with conventional staging and its impact on treatment decision making. J Nucl Med. 2003; 44:1784–1788. PMID: 14602860.3. Israel O, Yefremov N, Bar-Shalom R, et al. PET/CT detection of unexpected gastrointestinal foci of 18F-FDG uptake: incidence, localization patterns, and clinical significance. J Nucl Med. 2005; 46:758–762. PMID: 15872347.4. Jadvar H, Schambye RB, Segall GM. Effect of atropine and sincalide on the intestinal uptake of F-18 fluorodeoxyglucose. Clin Nucl Med. 1999; 24:965–967. PMID: 10595478.
Article5. Abdel-Nabi H, Doerr RJ, Lamonica DM, et al. Staging of primary colorectal carcinomas with fluorine-18 fluorodeoxyglucose whole-body PET: correlation with histopathologic and CT findings. Radiology. 1998; 206:755–760. PMID: 9494497.
Article6. Keogan MT, Lowe VJ, Baker ME, McDermott VG, Lyerly HK, Coleman RE. Local recurrence of rectal cancer: evaluation with F-18 fluorodeoxyglucose PET imaging. Abdom Imaging. 1997; 22:332–337. PMID: 9107663.7. Huebner RH, Park KC, Shepherd JE, et al. A meta-analysis of the literature for whole-body FDG PET detection of recurrent colorectal cancer. J Nucl Med. 2000; 41:1177–1189. PMID: 10914907.8. Falk PM, Gupta NC, Thorson AG, et al. Positron emission tomography for preoperative staging of colorectal carcinoma. Dis Colon Rectum. 1994; 37:153–156. PMID: 8306836.
Article9. Gutman F, Alberini JL, Wartski M, et al. Incidental colonic focal lesions detected by FDG PET/CT. AJR Am J Roentgenol. 2005; 185:495–500. PMID: 16037527.
Article10. Kamel EM, Thumshirn M, Truninger K, et al. Significance of incidental 18F-FDG accumulations in the gastrointestinal tract in PET/CT: correlation with endoscopic and histopathologic results. J Nucl Med. 2004; 45:1804–1810. PMID: 15534047.11. Prabhakar HB, Sahani DV, Fischman AJ, Mueller PR, Blake MA. Bowel hot spots at PET-CT. Radiographics. 2007; 27:145–159. PMID: 17235004.
Article12. Ahmad Sarji S. Physiological uptake in FDG PET simulating disease. Biomed Imaging Interv J. 2006; 2:e59. PMID: 21614339.
Article13. Tatlidil R, Jadvar H, Bading JR, Conti PS. Incidental colonic fluorodeoxyglucose uptake: correlation with colonoscopic and histopathologic findings. Radiology. 2002; 224:783–787. PMID: 12202714.
Article14. Kresnik E, Mikosch P, Gallowitsch HJ, Heinisch M, Lind P. F-18 fluorodeoxyglucose positron emission tomography in the diagnosis of inflammatory bowel disease. Clin Nucl Med. 2001; 26:867. PMID: 11564929.
Article15. Chen YK, Kao CH, Liao AC, Shen YY, Su CT. Colorectal cancer screening in asymptomatic adults: the role of FDG PET scan. Anticancer Res. 2003; 23:4357–4361. PMID: 14666651.16. Pandit-Taskar N, Schöder H, Gonen M, Larson SM, Yeung HW. Clinical significance of unexplained abnormal focal FDG uptake in the abdomen during whole-body PET. AJR Am J Roentgenol. 2004; 183:1143–1147. PMID: 15385321.
Article17. Strauss LG, Klippel S, Pan L, Schönleben K, Haberkorn U, Dimitrakopoulou-Strauss A. Assessment of quantitative FDG PET data in primary colorectal tumours: which parameters are important with respect to tumour detection? Eur J Nucl Med Mol Imaging. 2007; 34:868–877. PMID: 17219134.
Article18. Weston BR, Iyer RB, Qiao W, Lee JH, Bresalier RS, Ross WA. Ability of integrated positron emission and computed tomography to detect significant colonic pathology: the experience of a tertiary cancer center. Cancer. 2010; 116:1454–1461. PMID: 20143447.19. Isobe K, Hata Y, Sakaguchi S, et al. The role of positron emission tomography in the detection of incidental gastrointestinal tract lesions in patients examined for lung cancer. Nihon Kokyuki Gakkai Zasshi. 2010; 48:482–487. PMID: 20684209.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Comparison Study of Esophageal Findings on 18F-FDG PET/CT and Esophagogastroduodenoscopy
- Benign Colonic 18F-FDG Uptake on Whole-Body FDG-PET Scan
- Imaging Findings and Literature Review of 18F-FDG PET/CT in Primary Systemic AL Amyloidosis
- Colonic Uptake Patterns of F-18-FDG PET in Asymptomatic Adults: Comparison with Colonoscopic Findings
- Uptake of 18F-FDG in the Angioleiomyoma of the Leg
