Evaluation of the Cause of Internal Jugular Vein Obstruction on Head and Neck Contrast Enhanced 3D MR Angiography Using Contrast Enhanced Computed Tomography
- Affiliations
-
- 1Department of Diagnostic Radiology, Gangnam Severance Hospital, Yonsei University Health System, Korea. tschung@yuhs.ac
- KMID: 2041226
- DOI: http://doi.org/10.13104/jksmrm.2011.15.1.41
Abstract
- PURPOSE
To evaluate the cause of internal jugular vein (IJV) obstruction on contrast enhanced 3D MR angiography (CE-MRA) using contrast enhanced computed tomography (CE-CT).
MATERIALS AND METHODS
A total number of 30 patients were enrolled, who underwent both head and neck CE-MRA and CE-CT from 2005 to 2008. We defined obstruction group which had IJV obstruction and control group which had no IJV obstruction on CE-MRA. The following parameters were measured from axial images of CE-CT: 1) diameter of IJV; 2) distance between the styloid process and ipsilateral lateral mass of the atlas; 3) maximum area of lateral mass of the atlas. Each parameter was compared between obstruction group and control group.
RESULTS
The diameter of IJV and distance between the styloid process and lateral mass of the atlas at IJV obstruction side in obstruction group were 1.6 +/- 1.0 mm and 4.1 +/- 2.1 mm respectively, which resulted in statistical significance (p<0.01). The maximum area of lateral mass of the atlas at IJV obstruction side in obstruction group was 103.4 +/- 25.3 mm2 which is significantly larger than in control group (p<0.05).
CONCLUSION
We found that the cause of IJV obstruction on CE-MRA could be narrow space between the styloid process and the lateral mass of the atlas, which was related with asymmetric larger area of lateral mass of atlas.
Figure
-

Fig. 1 Each parameters were obtained from axial images of neck contrast-enhanced CT (a) Measurements calipers placed at the region of IJV at the level of maximum area of lateral mass of atlas. (b) Measurements calipers placed at the distance between styloid process and lateral mass of atlas at the level of maximum area of lateral mass of atlas. (c) Measuring the cross-sectional 2D area of maximum area of lateral mass of atlas.

Fig. 2 In obstruction group, (a) Neck contrast-enhanced MR angiography showing presence of internal jugular vein obstruction at left side (arrow). (b) Axial image of neck contrast-enhanced CT shows the narrower IJV diameter and distance between styloid process and lateral mass of atlas at left (arrow) than right side, and larger area of lateral mass of atlas at left than right side. (c) Sagittal image of neck contrast enhanced CT shows the no narrowing right IJV. (d) Sagittal image of neck contrast enhanced CT shows the narrowing left IJV at the level of betweeb styloid process and lateral mass of atlas (arrow).
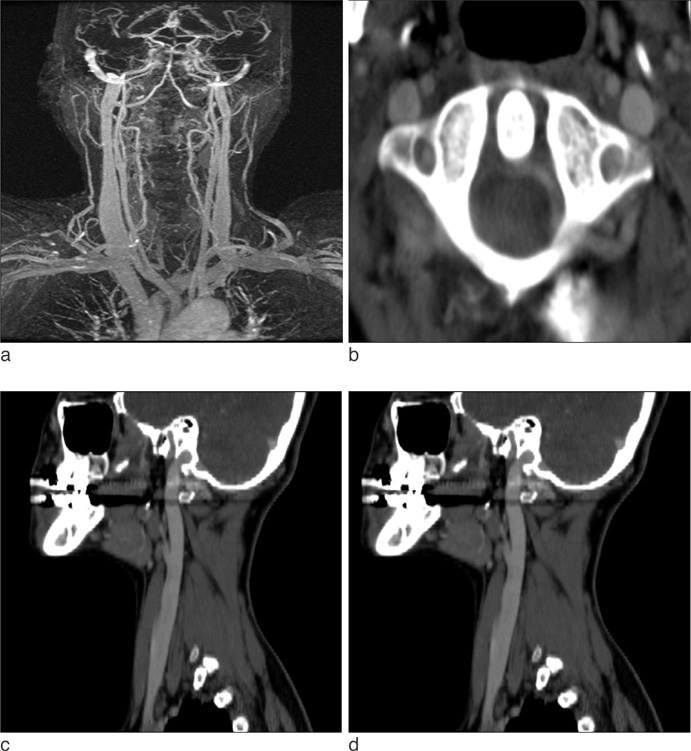
Fig. 3 In control group, (a) Neck contrast-enhanced MR angiography showing absence of internal jugular vein obstruction. (b) Axial image of neck contrast enhanced CT shows the no narrowing of IJV of both sides. (c, d) Sagittal images of neck contrast enhanced CT show the no narrowing of IJV of both sides (c: right, d: left)

Fig. 4 Graph of correlation between IJV diameter and distance between styloid process and lateral mass of atlas at IJV obstruction side in obstruction group. The diameter of IJV correlated well with distance between styloid process and lateral mass of atlas (R=0.942, p<0.001) at obstruction side in obstruction group.
Reference
-
1. Seoane E, Rhoton AL Jr. Compression of the internal jugular vein by the transverse process of the atlas as the cause of cerebellar hemorrhage after supratentorial craniotomy. Surg Neurol. 1999. 51:500–505.2. Gabella G. Williams P, editor. Cardiovascular system. Gray's Anatomy. 1995. London: Churchill Livingstone;1579–1580.3. Tedeschi H, Rhoton AL Jr. Lateral Approaches to the petroclival region. Surg Neurol. 1994. 41:180–216.4. Gooding CA, Stimac GK. Jugular vein obstruction caused by turning of the head. AJR Am J Roentgenol. 1984. 142:403–406.5. Standefer M, Bay JW, Trusso R. The sitting position in neurosurgery: a retrospective analysis of 488 cases. Neurosurgery. 1984. 14:649–658.6. Chandler JR. Diagnosis and cure of venous hum tinnitus. Laryngoscope. 1983. 93:892–895.7. Nehru VI, al-Khaboori MJ, Kishore K. Ligation of the internal jugular vein in hum tinnitus. J Laryngol Otol. 1993. 107:1037–1038.8. Bosnjak R, Kordas M. Circulatory effects of internal jugular vein compression: a computer simulation study. Med Biol Eng Comput. 2002. 40:423–431.9. Doepp F, Schreiber SJ, Dreier JP, Einhaupl KM, Valdueza JM. Migraine aggravation caused by cephalic venous congestion. Headache. 2003. 43:96–98.10. Alperin N, Lee SH, Mazda M, et al. Evidence for the importance of extracranial venous flow in patients with idiopathic intracranial hypertension (IIH). Acta Neurochir Suppl. 2005. 95:129–132.11. Piagkou M, Anagnostopoulou S, Kouladouros K, Piagkos G. Eagle's syndrome: a review of the literature. Clin Anat. 2009. 22:545–558.12. Ghosh LM, Dubey SP. The syndrome of elongated styloid process. Auris Nasus Larynx. 1999. 26:169–175.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Lemierre's Syndrome, Misdiagnosed as a Simple Deep Neck Infection on Initial Ultrasonography Followed by an Abscess Aspiration Trial
- A Case of Pancreatic Pseudoaneurysm with Aterio-venous Fistula in Acute Pancreatitis
- A Case of External Jugular Vein Thrombophlebitis with Sepsis
- Lemierre's Syndrome Following Acute Tonsillitis
- Preparative fasting before contrast-enhanced computed tomography
