J Korean Surg Soc.
2009 Jan;76(1):36-42. 10.4174/jkss.2009.76.1.36.
Clinical Experiences of Fitz-Hugh-Curtis Syndrome
- Affiliations
-
- 1Department of Surgery, Seoul Medical Center, Seoul, Korea. shinedk@seoulmc.or.kr
- 2Department of Radiology, Seoul Medical Center, Seoul, Korea.
- KMID: 2040602
- DOI: http://doi.org/10.4174/jkss.2009.76.1.36
Abstract
- PURPOSE
Fitz-Hugh-Curtis (FHC) syndrome has been described as perihepatitis associated with pelvic inflammatory disease during surgery. Recently, on computerized tomography a linear enhancement of the liver capsule was detected in a patient with FHC syndrome. We studied to evaluate the clinical course of the disease.
METHODS
Sixteen patients diagnosed with FHC syndrome from CT findings were retrospectively studied from April, 2006 to June, 2008.
RESULTS
The mean age of the patients was 25.9 (19~35) years and mean duration of abdominal pain was 3.9 (1~14) days. The most common complaint was right upper quadrant area pain (11 cases, 68.8%). 12 patients showed leukocytosis and all the patients had elevated serum C-reative protein levels. All the patients had normal liver function. Among the 9 patients which had polymerase chain reaction test for sexually transmitted disease (Chlamydia trachomatis, Ureaplasma urealyticum, Neisseria gonorrheae, Mycoplasma hominis), all showed more than one positive results (Chlamydia trachomatis 6 cases, Ureaplasma urealyticum 6 cases, Mycoplasma hominis 2 cases). On simple abdomen X-ray, 7 cases (43.8%) showed paralytic ileus. 14 cases received only antibiotic treatment, but 1 case had to take operation (laparoscopic-assisted adhesiolysis) due to constant abdominal pain and prolonged ileus.
CONCLUSION
It is important to rule out FHC syndrome by using CT findings, especially young women with right upper abdominal pain and PID. Usually, FHC syndrome can be treated easily with proper antibiotics.
MeSH Terms
-
Abdomen
Abdominal Pain
Anti-Bacterial Agents
Chlamydia Infections
Female
Gonorrhea
Hepatitis
Humans
Ileus
Intestinal Pseudo-Obstruction
Leukocytosis
Liver
Mycoplasma
Mycoplasma hominis
Neisseria
Pelvic Inflammatory Disease
Peritonitis
Polymerase Chain Reaction
Retrospective Studies
Sexually Transmitted Diseases
Ureaplasma urealyticum
Anti-Bacterial Agents
Chlamydia Infections
Hepatitis
Pelvic Inflammatory Disease
Peritonitis
Figure
-
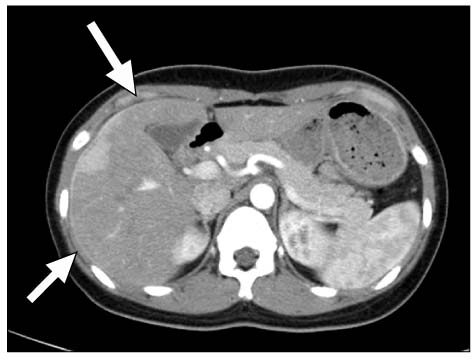
Fig. 1 Abdominopelvic CT arterial phase. Linear subcapsular enhancement at the anterior surface of the liver (arrow).
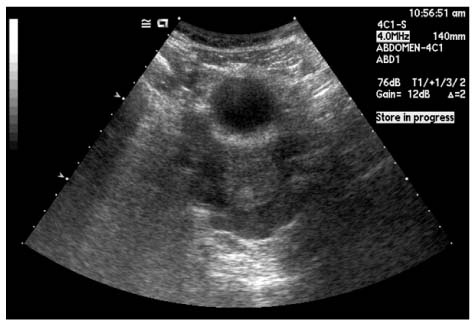
Fig. 2 Sonographic finding of pelvic fluid collection.

Fig. 3 Operative finding of hepatic capsular inflammation with adhesion of capsule to peritoneum.
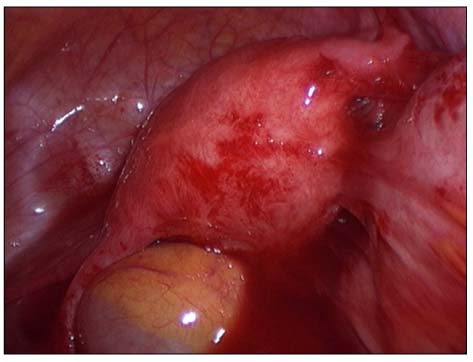
Fig. 4 Operative finding of pelvic inflammation with adhesion of uterus to ileum.
Reference
-
1. Peter NG, Clark LR, Jaeger JR. Fitz-Hugh-Curtis syndrome: a diagnosis to consider in women with right upper quadrant pain. Cleve Clin J Med. 2004. 71:233–239.2. Fitz-Hugh T Jr. Acute gonococcic peritonitis of the right upper quadrant in women. JAMA. 1934. 102:2094–2096.3. Curtis AH. A cause of adhesions in the right upper quadrant. JAMA. 1930. 94:1221–1222.4. Muller-Schoop JW, Wang SP, Munzinger J, Schlapfer HU, Knoblauch M, Tammann RW. Chlamydia trachomatis as possible cause of peritonitis and perihepatitis in young women. Br Med J. 1978. 1:1022–1024.5. Wang SP, Eschenbach DA, Holmes KK, Wager G, Grayston JT. Chlamydia trachomatis infection in Fitz-Hugh-Curtis syndrome. Am J Obstet Gynecol. 1980. 138:1034–1038.6. Lopes-Zeno JA, Keith LG, Berger GS. The Fitz-Hugh-Curtis syndrome revisited: changing perspectives after half a century. J Reprod Med. 1985. 30:567–582.7. Sharma JB, Roy KK, Gupta N, Jain SK, Malhotra N, Mittal S. High prevalence of Fitz-Hugh-Curtis syndrome in genital tuberculosis. Int J Gynecol Obstet. 2007. 99:62–63.8. Nishie A, Yoshimiusu K, Irie H, Yoshitake T, Aibe H, Tajima T, et al. Fitz-Hugh-Curtis syndrome radiologic manifestation. J Comput Assist Tomogr. 2003. 27:786–791.9. Oh JH, Cho YS, Choi YH, Lee HS. A diagnostic utility of Fitz-Hugh-Curtis syndrome by using contrast enhanced abdominopelvic computerized tomography. J Korean Soc Emerg Med. 2005. 16:410–415.10. Jin SC, Sohn YD, Choi WI. Two cases of Fitz-Hugh-Curtis syndrome diagnosed by abdominopelvic computerized tomography. Keimyung Med J. 2006. 26:52–56.11. Lee SC, Nah BG, Kim HS, Choi TH, Lee SH, Lee JY, et al. Two cases of Fitz-Hugh-Curtis syndrome in acute phase. Korean J Gastroenterol. 2005. 45:137–142.12. Zeger W, Holt K. Gynecologic infections. Emerg Med Clin North Am. 2003. 21:631–648.13. Tsubuku M, Hayashi S, Terahara A, Furukawa T, Ohmura G. Fitz-Hugh-Curtis syndrome: linear contrast enhancement of the surface of the liver on CT. J Comput Assist Tomogr. 2002. 26:456–458.14. Kechagia N, Bersimis S, Chatzipanagiotou S. Incidence and antimicrobial susceptibilities of genital mycoplasmas in outpatient women with clinical vaginitis in Athens, Greece. J Antimicrob Chemother. 2008. 62:122–125.15. McCormick M, DelCastillo J, Berk RS. An atypical presentation of the Fitz-Hugh-Curtis syndrome. J Emerg Med. 1990. 8:55–58.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Fitz-Hugh-Curtis syndrome in a male patient
- A case of Fitz-Hugh-Curtis syndrome diagnosed by pelvic CT imaging prior to diagnostic laparoscopy
- Inflammatory Pseudotumor in the Liver and Right Omentum Caused by Pelvic Inflammatory Disease: A Case Report
- Two Cases of Fitz - Hugh - Curtis Syndrome Associated with Ectopic Pregnancy
- A Case of Fitz-Hugh-Curtis Syndrome
