Radiological Imaging of Aortic Aneurysms
- Affiliations
-
- 1Department of Diagnostic Radiology, Kyungpook National University Hospital, Daegu, Korea. jonglee@knu.ac.kr
- KMID: 2029060
- DOI: http://doi.org/10.4070/kcj.2007.37.8.337
Abstract
- The development of radiological equipment such as MDCT or ultrasonography has increased the diagnostic accuracy of aortic aneurysms and has allowed for improvements in surgical and interventional treatment techniques. However, the mortality and morbidity rate of aortic aneurysms has not decreased significantly. For this reason, there is continuous interest in radiological evaluations of aortic aneurysms. This report reviews the radiological image findings and useful indications for both the diagnosis and surveillance of aortic aneurysms. The popular radiological features of an aortic aneurysm are aortic expansion, combined atherosclerosis, intraluminal mural thrombus, perianeurysmal inflammation and fibrosis, and perianeurysmal hemorrhage due to rupture. As rupture is the most important complication of an aortic aneurysm, various signs of an impending rupture have been suggested. These include the following: a maximum aneurysmal diameter larger than the threshold value, a high expansion rate, periaortic sentinel hemorrhage, and a hyperattenuating crescent in the mural thrombus or aneurysmal wall. To acknowledge the impending rupture of an aortic aneurysm, careful depiction of the clues is indispensable.
MeSH Terms
Figure
-
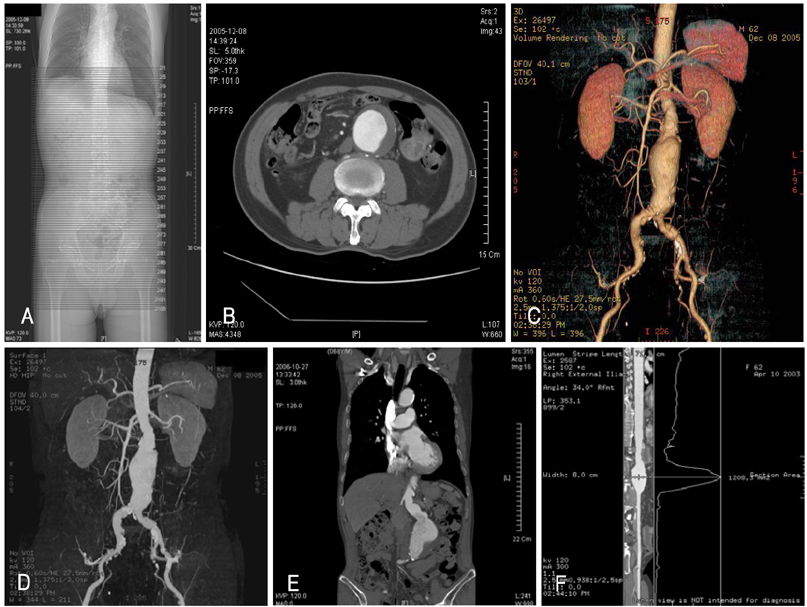
Fig. 1 Imaging of an abdominal aortic aneurysm using 16-channel multi-detector computed tomography (MDCT) and post-processing techniques. A: scan planning on a scout image was from above the diaphragm down to the perineum, with a slice thickness of 5 mm. A total of 105 axial images were obtained using this plan. B: basic reconstruction of an axial image with a slice thickness of 5 mm shows an abdominal aortic aneurysm and intraluminal mural thrombus. Some calcification can be seen at the outer aneurysmal wall toward the mural thrombus. C: a three-dimensional reconstruction, volume rendering (VR) technique, showing an expanded lumen of the abdominal aortic aneurysm along with neighboring anatomical structures such as renal and iliac arteries. The distance between the upper end of the aneurysm and orifice of the right renal artery, the "proximal leg", was measured as 3.3 cm. Also noted is the wall calcification in the abdominal aortic aneurysm and both iliac arteries. D: the maximum intensity projection (MIP) technique contains three-dimensional information converted into a two-dimensional image. The sequential multiple angle display is useful for depicting the three-dimensional information. E: coronal reconstruction using multiplanar reformatting (MPR) clearly shows the relationship between the abdominal aortic aneurysm and renal arterial orifices. F: a curved MPR was produced along the whole length of the scanned aorta and iliofemoral artery. The displayed image shows a straightened aortoiliofemoral artery and cross-sectional area curve at the horizontally matched level.

Fig. 2 Magnetic resonance imaging (MRI) of an abdominal aortic aneurysm. A: a contrast-enhanced three-dimensional fast gradient echo technique acquired coronal image of an abdominal aortic aneurysm. The irregular luminal contour suggests the presence of atherosclerotic plaque. B: Post-processing of the raw image data, using maximum intensity projection (MIP), reveals an abdominal aortic aneurysm involving the area from the renal arterial orifice to both iliac arteries. The right common iliac artery shows a complete occlusion.
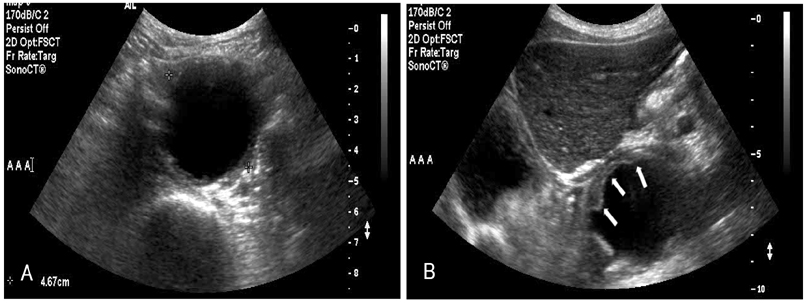
Fig. 3 Ultrasonographic images of the abdominal aortic aneurysm. A: transverse B-mode ultrasonography, using a 5-2 MHz transducer, shows a 4.67 cm sized aneurysm. B: in the oblique scan, the presence of a mural thrombus (arrows) is remarkable within the aortic aneurysmal lumen located under the left hepatic lobe.

Fig. 4 Transarterial aortography of an abdominal aortic aneurysm. A: through the right common femoral artery, a 5-French catheter was inserted up to the proximal abdominal aorta and iodinated contrast media was injected during the repeated image acquisitions. The abdominal aortic aneurysm and its location could be identified, but the precise morphology and size of the aneurysm could not be depicted due to the obscure margin of contrast-filled lumen. B: through the bilateral common femoral arteries, a bifurcated stent-graft was inserted successfully across the aneurysm. No more abdominal aortic aneurysm was observed, and well-reconstructed aortic lumens could be identified.
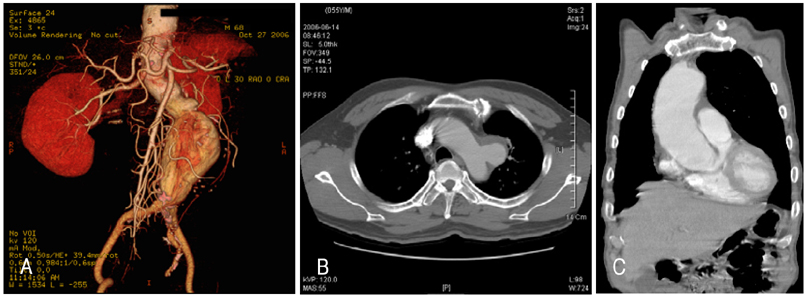
Fig. 5 Various shapes of an aortic aneurysm. A: a fursiform aneurysm developed in the lower abdominal aorta. The image shows a long proximal leg but no distal leg, between the lower end of the aneurysm as well as aortoiliac bifurcation. In addition, there is angulation of the abdominal aorta. B: a saccular aneurysm is depicted in the distal aortic arch at its left lateral aspect. An mural thrombus located in the anterior aspect and posterior aspect of the aneurysmal neck shows a more acute angle, possibly due to hemodynamic stress. C: coronal multiplanar reformatting reveals a cylindroid aneurysm located at the ascending aorta.

Fig. 6 An axial computed tomography (CT) image at the level of the thoracic descending aorta reveals an aortic aneurysm and remarkable calcified atherosclerotic plaque. A mural thrombus is located in the inner side of the calcified plaque. The presence of perianeurysmal soft tissue and fluid density suggests a concealed rupture. Reactive left pleural effusion can also be seen.

Fig. 7 An axial computed tomography (CT) image shows a 71 mm sized abdominal aortic aneurysm and a remarkable mural thrombus located in the aneurysmal lumen. Perianeurysmal inflammatory granulation tissue is depicted as a soft tissue mass with adhesion to the adjacent structures (arrows).
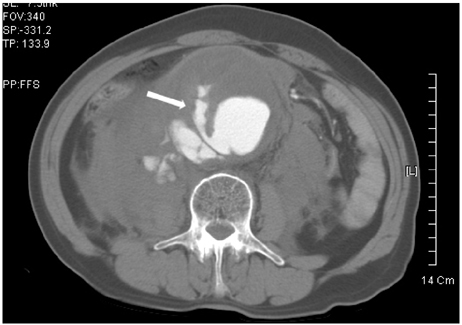
Fig. 8 Abdominal computed tomography (CT) angiography reveals a ruptured abdominal aortic aneurysm. The maximum diameter of the aneurysm was measured as 90.8 mm. The lumen of the aneurysm is located eccentrically at the right posterolateral aspect and the aneurysmal wall shows marked thinning. A finger-like extravasation of luminal contrast media (arrow) is noted through the mural thrombus and aneurysmal wall suggesting a rupture. Perianeurysmal accumulation of the contrast media also suggests a ruptured aneurysmal wall. A large hematoma can be seen in the retroperitoneal space.
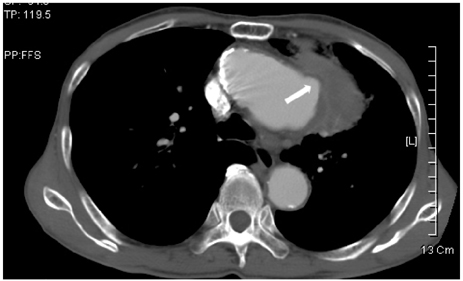
Fig. 9 An ascending aortic aneurysm is depicted in a contrast-enhanced computed tomography (CT) image. There is focal outpouching of the aneurysmal lumen, and an aortic bleb in the left lateral side and a small amount of perianeurysmal hemorrhage. These findings can be regarded as impending rupture signs.

Fig. 10 A 65-year-old male with a complaint of acute onset radiating back pain was scanned by computed tomography (CT). An abdominal aortic aneurysm is depicted along with a retroperitoneal hemorrhage suggesting a ruptured aneurysm. A mural thrombus is noted at the ventral aspect of the aneurysm and a hyperdense crescent sign due to an acute hemorrhage can be seen within the thrombus (arrow).
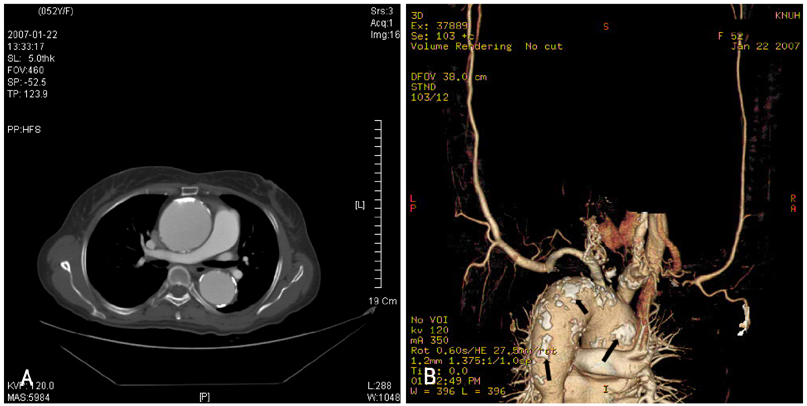
Fig. 11 A thoracic aortic aneurysm superimposed on chronic Takayasu aortitis. A: a cylindroid aneurysm developed from the ascending aorta to the proximal thoracic descending aorta. Transmural calcification spots located at the aneurysmal wall indicate underlying chronic Takayasu aortitis. B: right posterolateral view of the volume-rendering image reveals multiple patchy calcification along the aortic wall (arrows). The distal thoracic descending aorta shows stenosis as a sign of chronic Takayasu aortitis.
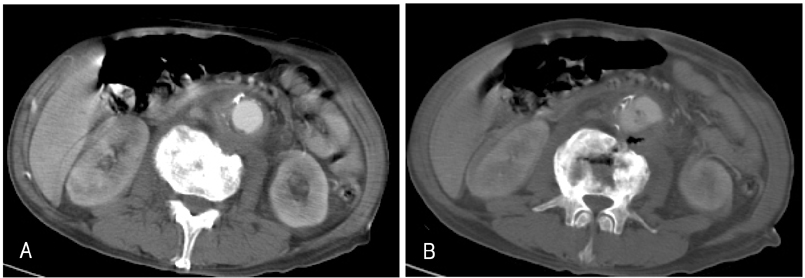
Fig. 12 An abdominal computed tomography (CT) image of a 67-year-old male shows an infected aortic aneurysm. A: mild dilatation of the abdominal aorta, periaortic inflammatory granulation tissue, and destructive changes in the adjacent vertebral body indicate an infected abdominal aortic aneurysm. B: air bubbles can be seen at the aneurysmal wall, perianeurysmal granulation tissue area, and destroyed vertebral body suggesting an infection by a gas-forming agent.
Reference
-
1. Sakalihasan N, Limet R, Defawe OD. Abdominal aortic aneurysm. Lancet. 2005. 365:1577–1589.2. Sanfelippo PM. Abdominal aortic aneurysm-2003: what we know, what we don't know. Int J Angiol. 2003. 2:145–152.3. van der Vliet JA, Boll AP. Abdominal aortic aneurysm. Lancet. 1997. 349:863–866.4. McGregor JC, Pollock JG, Anton HC. The value of ultrasonography in the diagnosis of abdominal aortic aneurysm. Scott Med J. 1975. 20:133–137.5. Macura KJ, Corl FM, Fishman EK, Bluemke DA. Pathogenesis in acute aortic syndromes: aortic aneurysm leak and rupture and traumatic aortic transaction. AJR Am J Roentgenol. 2003. 181:303–307.6. Armerding MD, Rubin GD, Beaulieu CF, et al. Aortic aneurysmal disease: assessment of stent-graft treatment-CT versus conventional angiography. Radiology. 2000. 215:138–146.7. Anbarasu A, Harris PL, McWilliams RG. The role of gadolinium-enhanced MR imaging in the preoperative evaluation of inflammatory abdominal aortic aneurysm. Eur Radiol. 2002. 12:S192–S195.8. Mueller-Mang C, Wunderbaldinger P, Janata-Schwatzek K, Schoder M, Roegler M, Bankier AA. Acute dissection and contained rupture of a thoracic aortic aneurysm: emergency diagnosis with nonenhanced MR angiography. Cardiovasc Intervent Radiol. 2006. 29:930–933.9. Pereles FS, McCarthy RM, Baskaran V, et al. Thoracic aortic dissection and aneurysm: evaluaiton with nonenhanced true FISP MR angiography in less than 4 minutes. Radiology. 2002. 223:270–274.10. Quill DS, Colgan MP, Sumner DS. Ultrasonic screening for the detection of abdominal aortic aneurysms. Surg Clin North Am. 1989. 69:713–720.11. Catalano O, Lobianco R, Cusati B, Siani A. Contrast-enhanced sonography for diagnosis of ruptured abdominal aortic aneurysm. AJR Am J Roentgenol. 2005. 184:423–427.12. Siegel CL, Cohan RH. CT of abdominal aortic aneurysms. AJR Am J Roentgenol. 1994. 163:17–29.13. Defawe OD, Colige A, Lambert CA, et al. TIMP-2 and PAI-1 mRNA levels are lower in aneurysmal as compared to atheroocclusive abdominal aortas. Cardiovasc Res. 2003. 60:205–213.14. Yamazumi K, Ojiro M, Okumura H, Aikou T. An activated state of blood coagulation and fibrinolysis in patients with abdominal aortic aneurysm. Am J Surg. 1998. 175:297–301.15. Lindholt JS, Jorgensen B, Fasting H, Henneberg EW. Plasma levels of plasmin-antiplasmin-complexes are predictive for small abdominal aortic aneurysms expanding to operation-recommendable sizes. J Vasc Surg. 2001. 34:611–615.16. Mukaiyama H, Shionoya S, Ikezawa T, Kamiya T, Hamaguchi M, Saito H. Abdominal aortic aneurysm complicated with chronic disseminated intravascular coagulopathy: a case of surgical treatment. J Vasc Surg. 1987. 6:600–604.17. Wang XF, Liu L, Cheng TO, Li ZA, Deng YB, Wang JE. The relationship between intracariovascular smoke-like echo and erythrocyte rouleaux formation. Am Heart J. 1992. 124:961–965.18. Schurink GW, van Baalen JM, Visser MJ, van Bockel JH. Thrombus within an aortic aneurysm does not reduce pressure on the aneurysmal wall. J Vasc Surg. 2000. 31:501–506.19. Di Martino E, Mantero S, Inzoli F, et al. Biomechanics of abdominal aortic aneurysm in the presence of endoluminal thrombus: experimental characterisation and structural static computational analysis. Eur J Vasc Endovasc Surg. 1998. 15:290–299.20. Mower WR, Quinones WJ, Gambhir SS. Effect of intraluminal thrombus on abdominal aortic aneurysm wall stress. J Vasc Surg. 1997. 26:602–608.21. Wang DH, Makaroun MS, Webster MW, Vorp DA. Effect of intraluminal thrombus on wall stress in patient-specific models of abdominal aortic aneurysm. J Vasc Surg. 2002. 36:598–604.22. Thubrikar MJ, Robicsek F, Labrosse M, Cherrenkoff V, Fowler BL. Effect of thrombus on abdominal aortic aneurysm wall dilatation and stress. J Cardiovasc Surg. 2003. 44:67–77.23. Hans SS, Jareunpoon O, Huang R, Hans B, Bove P, Zelenock GB. Relationship of residual intraluminal to intrathorombotic pressure in a closed aneurysmal sac. J Vasc Surg. 2003. 37:949–953.24. Takagi H, Yoshikawa S, Mizuno Y, et al. Intrathrombotic pressure of a thrombosed abdominal aortic aneurysm. Ann Vasc Surg. 2005. 19:108–112.25. Satta J, L ra E, Juvonen T. Intraluminal thrombus predicts rupture of an abdominal aortic aneurysm. J Vasc Surg. 1996. 23:737–739.26. Stenbaek J, Kalin B, Swedenborg J. Growth of thrombus may be a better predictor of rupture than diameter in patients with abdominal aortic aneurysms. Eur J Vasc Endovasc Surg. 2000. 20:466–469.27. Vorp DA, Wang DH, Webster MW, Federspiel WJ. Effect of intraluminal thrombus thickness and bulge diameter on the oxygen diffusion in abdominal aortic aneurysm. J Biomech Eng. 1998. 120:579–583.28. Fontaine V, Jacob MP, Houard X, et al. Involvement of the mural thrombus as a site of protease release and activation in human aortic aneurysms. Am J Pathol. 2002. 161:1701–1710.29. Sterpetti AV, Hunter WJ, Feldhaus RJ, et al. Inflammatory aneurysms of the abdominal aorta: incidence, pathologic, and etiologic considerations. J Vasc Surg. 1989. 9:643–650.30. Walker DI, Bloor K, Williams G, Grillie I. Inflammatory aneurysm of the abdominal aorta. Br J Surg. 1972. 59:609–614.31. Hayashi H, Hidaka F, Kumazaki T, Ochi M. Serial assessment of the development of inflammatory abdominal aorticaneurysm from ordinary atherosclerotic abdominal aortic aneurysm usingmultidetector-row computed tomographic angiography. Heart Vessels. 2006. 21:334–337.32. Rasmussen TE, Hallett JW. Inflammatory aortic aneurysms: a clinical review with new perspectives in pathogenesis. Ann Surg. 1997. 225:155–164.33. Iino M, Kuribayashi S, Imakita S, et al. Sensitivity and specificity of CT in the diagnosis of inflammatory abdominal aortic aneurysms. J Comput Assist Tomogr. 2002. 26:1006–1012.34. Errington ML, Ferguson JM, Gillespie IN, Conal HM, Ruckley CV, Wright AR. Complete pre-operative imaging assessment of abdominal aortic aneurysms with spiral CT angiography. Clin Radiol. 1997. 52:369–377.35. Latifi HR, Heiken JP. CT of inflammatory abdominal aortic aneurysm: development from an uncomplicated atherosclerotic aneurysm. J Comput Assist Tomogr. 1992. 16:484–486.36. Kittredge RD, Gordon R. Inflammatory aneurysm of aorta: development documented by computed tomography. J Comput Tomogr. 1987. 11:128–131.37. Rozenblit A, Bennett J, Suggs W. Evolution of the infected abdominal aortic aneurysm: CT observation of early aortitis. Abdom Imaging. 1996. 21:512–514.38. Gayer G, Bass A. Delayed rupture of abdominal aortic false aneurysm following blunt trauma. Emerg Radiol. 2003. 10:64–66.39. Burke DR. Baum A, editor. Aneurysms of the abdominal aorta. Abram's Angiography: Vascular and Interventional Radiology. 1997. 4th ed. Boston: Little, Brown and Company;1079–1080.40. Jones CS, Reilly MK, Dalsing MC, Glover JL. Chronic contained rupture of abdominal aortic aneurysms. Arch Surg. 1986. 121:542–546.41. Zarins CK, Hill BB, Wolf YG. Townsend CM, Beauchamp DR, Evers MB, Mattox KL, Sabiston DC, editors. Aneurysmal vascular disease. Sabiston Textbook of Surgery. 2001. 16th ed. Philadelphia: W.B.Saunders;1357–1372.42. Mehard WB, Heiken JP, Sicard GA. High-attenuating crescent in abdominal aortic aneurysm wall at CT: a sign of acute or impending rupture. Radiology. 1994. 192:359–362.43. Siegel CL, Cohan RH, Korobkin M, Alpern MB, Courneya DL, Leder RA. Abdominal aortic aneurysm morphology: CT features in patients with ruptured and nonruptured aneurysms. AJR Am J Roentgenol. 1994. 163:1123–1129.44. Nevitt M, Ballard D, Hallet J. Prognosis of abdominal aortic aneurysms: a population-based study. N Engl J Med. 1989. 321:1009–1014.45. Limet R, Sakalihassan N, Albert A. Determination of the expansion rate and incidence of rupture of abdominal aortic aneurysms. J Vasc Surg. 1991. 14:540–548.46. Arita T, Matsunaga N, Takano K, et al. Abdominal aortic aneurysm: rupture associated with the high-attenuating crescent sign. Radiology. 1997. 204:765–768.47. Schwartz SA, Taljanovic MS, Smyth S, O'Brien MJ, Rogers LF. CT findings of rupture, impending rupture, and contained rupture of abdominal aortic aneurysms. AJR Am J Roentgenol. 2007. 188:W57–W62.48. Halliday KE, Al-Kutoubi A. Draped aorta: CT sign of contained leak of aortic aneurysms. Radiology. 1996. 199:41–43.49. Kieffer E, Chiche L, Bertal A, et al. Descending thoracic and thoracoabdominal aortic aneurysm in patients with Takayasu's disease. Ann Vasc Surg. 2004. 18:505–513.50. Takagi A, Tada Y, Ueno A. Greenhalgh RM, Mannick JA, editors. An extension of the classification of Takayasu's disease and the management of inflammatory aneurysm in Japan. The Cause and Management of Aneurysms. 2000. London: WB Saunders;213–219.51. Subramanyan R, Joy J, Balakrishnan KG. Natural history of aortoarteritis (Takayasu's disease). Circulation. 1989. 80:429–437.52. Macedo TA, Stanson AW, Oderich GS, Johson CM, Panneton JM, Tie ML. Infected aortic aneurysms: imaging findings. Radiology. 2004. 231:250–257.53. Gomes MN, Choyke PL. Infected aortoic aneurysms of the aorta: CT diagnosis. J Cardiovasc Surg. 1992. 33:684–689.54. Oderich GS, Panneton JM, Bower TC, et al. Infected aortic aneurysms: aggressive presentation, complicated early outcome, but durable results. J Vasc Surg. 2001. 34:900–908.55. Bennett DE. Primary mycotic aneurysms of the aorta: report of case and review of the literature. Arch Surg. 1967. 94:758–765.56. Perry MO. Infected aortic aneurysms. J Vasc Surg. 1985. 2:597–599.57. Aliaga L, Cobo F, Miranda C, Lara J. Mycotic aneurysm of the aortic arch. Infection. 2000. 28:240–242.58. Castaneda-Zuniga WR, Nath PH, Zollikofer C, Velasquez G, Valdez-Davila O, Edwards E. Mycotic aneurysm of the aorta. Cardiovasc Intervent Radiol. 1980. 3:144–149.59. Kaufman SL, White RI Jr, Harrington DP, Barth KH, Siegelman SS. Protean manifestations of mycotic aneurysms. AJR Am J Roentgenol. 1978. 131:1019–1025.60. Bennett DE, Cherry JK. Bacterial infection of aortic aneurysm: a clinicopathologic study. Am J Surg. 1967. 113:321–326.61. Baltacioglu F, Cunsit NC, Aribal ME. Tuberculous abdominal aortic aneurysm in a 14-year-old child. Pediatr Radiol. 1999. 29:536–538.62. Rozenblit A, Wasserman E, Marin ML, Veith FJ, Cynamon J, Rozenblit G. Infected aortic aneurysm and vertebral osteomyelitis after intravesical Bacillus-Calmette-Gue'rin therapy. AJR Am J Roentgenol. 1996. 167:711–713.63. Sueyoshi E, Sakamoto I, Kawahara Y, Matsuoka Y, Hayashi K. Infected abdominal aortic aneurysm: early CT findings. Abdom Imaging. 1998. 23:645–648.64. Yasuhara H, Muto T. Infected abdominal aortic aneurysm presenting with sudden appearance: diagnostic importance of serial computed tomography. Ann Vasc Surg. 2001. 15:582–585.65. Bower TC, Cherry KJ Jr, Pairolero PC. Unusual manifestations of abdominal aortic aneurysms. Surg Clin North Am. 1989. 69:745–754.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hrombosed Aortic Dissections and Aortic Aneurysms: MRI Findings and Differential Diagnosis
- MR Findings of Thoracic and Abdominal Aortic Aneurysms: Comparison with Anglographic and Surgical Findings
- Aortic Arch Aneurysm: CT and MR Features
- Aortic Valve Sparing Operations: A Review
- Multiple Intracranial Aneurysms Associated with Interrupted Aortic Arch
