Fatal Delayed Coronary Artery Perforation After Coronary Stent Implantation
- Affiliations
-
- 1Department of Cardiology, CHA Bundang Medical Center, CHA University, Seongnam, Korea. answodus@medimail.co.kr
- KMID: 2028766
- DOI: http://doi.org/10.4070/kcj.2012.42.5.352
Abstract
- Most type I and II perforations are predominately caused by hydrophilic and stiff wires, often presented in the delayed form, and do not require pericardial drainage or surgical interventions. However, we report a type III delayed coronary artery perforation at the site of stent implantation after intervention without any evidence of immediate perforations. To the best of our knowledge, this is the first case report of angiographic documentation and treatment of delayed coronary perforation at the site of stent, presented as a cardiac arrest.
Keyword
MeSH Terms
Figure
-
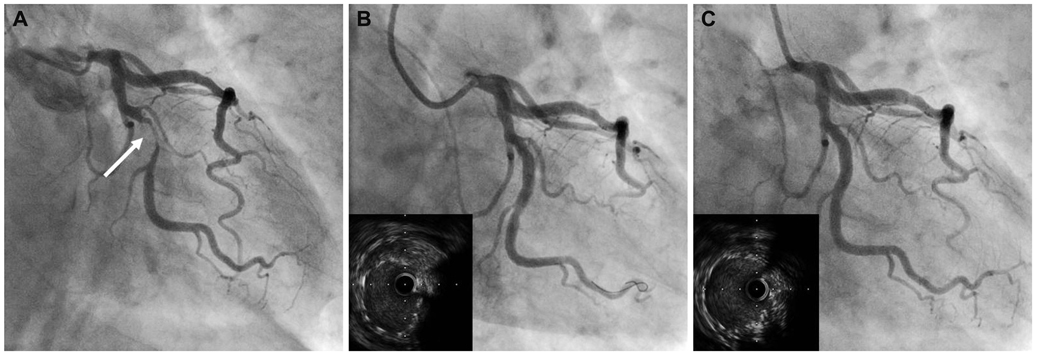
Fig. 1 Coronary angiogram for pecutaneous coronary intervention for critical stenosis of left. Circumflex artery. A: coronary angiogram showed critical stenosis of left circumflex artery (arrow). B: after stenting, angiogram showed mild residual stenosis in proximal stented lesion and intravascular ultrasound showed incomplete expansions. C: final angiogram showed no residual lesion and final intravascular ultrasound images revealed improved expansion and good apposition of the stent.

Fig. 2 Coronary angiogram after cardiovascular resuscitation due to sudden cardiac arrest in general ward. A: angiogram showed type III coronary perforation with bleeding at the previous stent implantation site (arrow). B: before inflation, first Jo graft stent was placed for the active bleeding site. C: after stenting of two graft stents, the final angiogram during cardiovascular resuscitation showed no additional bleeding.
Reference
-
1. Ellis SG, Ajluni S, Arnold AZ, et al. Increased coronary perforation in the new device era: incidence, classification, management, and outcome. Circulation. 1994. 90:2725–2730.2. Gunning MG, Williams IL, Jewitt DE, Shah AM, Wainwright RJ, Thomas MR. Coronary artery perforation during percutaneous intervention: incidence and outcome. Heart. 2002. 88:495–498.3. Gruberg L, Pinnow E, Flood R, et al. Incidence, management, and outcome of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol. 2000. 86:680–682.4. Shimony A, Zahger D, Van Straten M, et al. Incidence, risk factors, management and outcomes of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol. 2009. 104:1674–1677.5. Von Sohsten R, Kopistansky C, Cohen M, Kussmaul WG 3rd. Cardiac tamponade in the "new device" era: evaluation of 6999 consecutive percutaneous coronary interventions. Am Heart J. 2000. 140:279–283.6. Fasseas P, Orford JL, Panetta CJ, et al. Incidence, correlates, management, and clinical outcome of coronary perforation: analysis of 16,298 procedures. Am Heart J. 2004. 147:140–145.7. Fukutomi T, Suzuki T, Popma JJ, et al. Early and late clinical outcomes following coronary perforation in patients undergoing percutaneous coronary intervention. Circ J. 2002. 66:349–356.8. Ramana RK, Arab D, Joyal D, et al. Coronary artery perforation during percutaneous coronary intervention: incidence and outcomes in the new interventional era. J Invasive Cardiol. 2005. 17:603–605.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Coronary Artery Perforation Following Implantation of a Drug-Eluting Stent Rescued by Deployment of a Covered Stent in Symptomatic Myocardial Bridging
- Aspiration Thromboembolectomy in the Management of Acute Coronary Occlusion during Pertaneous Transluminal Coronary Angioplasty
- Treatment of Coronary Artery Perforation and Tamponade Complicating Balloon Angioplasty by PTFE-Covered Stent. A Case Report
- A Case of Coronary Artery Aneurysm after Sirolimus-Eluting Stent Implantation
- Successful Treatment of a Coronary Artery Aneurysm that Developed with In-Stent Restenosis after Drug-Eluting Stent Implantation
