Coronary Artery Perforation Following Implantation of a Drug-Eluting Stent Rescued by Deployment of a Covered Stent in Symptomatic Myocardial Bridging
- Affiliations
-
- 1Department of Cardiology, Fengtian Hospital Affiliated to Shenyang Medical College, Shenyang, Liaoning Province, China.
- 2Department of Cardiology, Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea. kangwch@gilhospital.com
- KMID: 2094077
- DOI: http://doi.org/10.4070/kcj.2010.40.3.148
Abstract
- We successfully rescued a patient whose coronary artery perforated following implantation of a drug-eluting stent (DES), by deploying a stent-graft in symptomatic myocardial bridging. Our case demonstrated that coronary perforation could be handled without difficulty when perforated myocardial bridging is confined to the interventricular groove
MeSH Terms
Figure
-
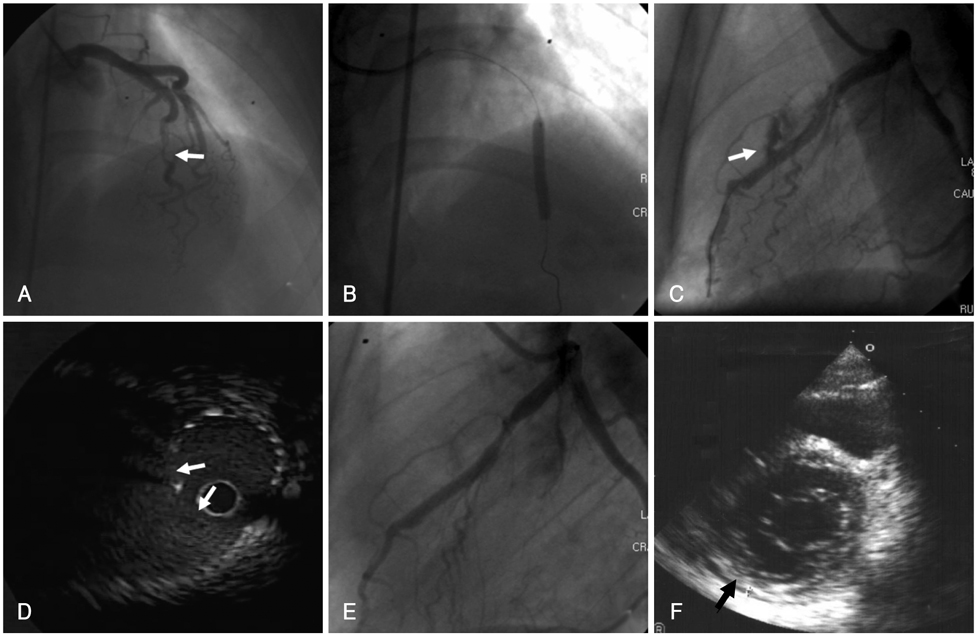
Fig. 1 A: angiography revealed 80% stenosis aggravated by severe muscular bridging at the mid LAD. B: at a nominal pressure of, the stent was not fully expanded in the middle segment of the lesion. So, we inflated the stent with a high pressure, up to 16 atm. C: on follow-up angiography, the coronary artery was perforated and extravasation of contrast into the pericardium was noted at the site of the lesion. D: an IVUS study showed the perforation site and a perivascular hematoma along the lesion. E: after implantation of a covered stent, leaking flow from the coronary lesion was no longer noted. F: follow-up echocardiography showed a minimal amount of pericardial effusion (arrow) without hemodynamic instability. LAD: left anterior descending, IVUS: intravascular ultrasound.
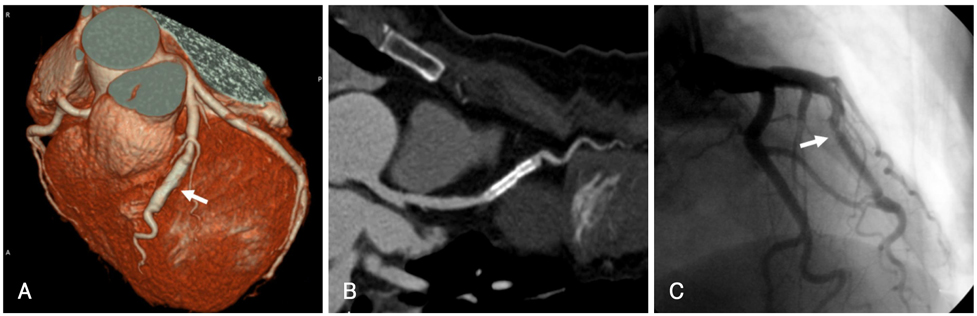
Fig. 2 A and B: four months after the stent procedure, CT angiography showed no evidence of residual hematoma or pseudoaneurysm (arrow). C: follow-up coronary angiography performed at 8 months after the procedure showed good distal flow with minimal stenosis at the proximal edge of the stent (arrow).
Reference
-
1. Tauth J, Sullebarger T. Myocardial infarction associated with myocardial bridging: case history and review of the literature. Cathet Cardiovasc Diagn. 1997. 40:364–367.2. Cutler D, Wallace JM. Myocardial bridging in a young patient with sudden death. Clin Cardiol. 1997. 20:581–583.3. Alegria JR, Herrmann J, Holmes DR Jr, Lerman A, Rihal CS. Myocardial bridging. Eur Heart J. 2005. 26:1159–1168.4. Mohlenkamp S, Hort W, Ge J, Erbel R. Update on myocardial bridging. Circulation. 2002. 106:2616–2622.5. Broderick TM, Kereiakes DJ, Whang DD, Toltzis RJ, Abbottsmith CW. Myocardial bridging may predispose to coronary perforation during rotational atherectomy. J Invasive Cardiol. 1996. 8:161–163.6. Hering D, Horstkotte D, Schwimmbeck P, Piper C, Bilger J, Schultheiss HP. Acute myocardial infarct caused by a muscle bridge of the anterior interventricular ramus: complicated course with vascular perforation after stent implantation. Z Kardiol. 1997. 86:630–638.7. Berry JF, von Mering GO, Schmalfuss C, Hill JA, Kerensky RA. Systolic compression of the left anterior descending coronary artery: a case series, review of the literature, and therapeutic options including stenting. Catheter Cardiovasc Interv. 2002. 56:58–63.8. Kim BJ, Gwon HC, Hong JS, et al. Clinical aspects of coronary artery perforation during percutaneous coronary intervention. Korean Circ J. 2003. 33:277–283.9. Haager PK, Schwartz ER, vom Dahl J, Klues HG, Reffelmann T, Hanrath P. Long term angiographic and clinical follow up in patients with stent implantation for symptomatic myocardial bridging. Heart. 2000. 84:403–408.10. Choi SH, Shim SJ, Byun KH, Choi D, Shim WH. A case of coronary stenting in the management of myocardial ischemia caused by myocardial bridging. Korean Circ J. 2001. 31:940–944.11. Morales AR, Romanelli R, Tate LG, Boucek RJ, de Marchena E. Intramural left anterior descending coronary artery: significance of the depth of the muscular tunnel. Hum Pathol. 1993. 24:693–701.12. Glagov S, Zarins C, Giddens DP, Ku DN. Hemodynamics and atherosclerosis: insights and perspectives gained from studies of human arteries. Arch Pathol Lab Med. 1988. 112:1018–1031.13. Qian J, Zhang F, Wu H, et al. Size of coronary artery in myocardial bridge compared with adjacent nontunneled left anterior descending coronary artery. Am J Cardiol. 2007. 99:1653–1655.14. Ajluni SC, Glazier S, Blankenship L, O'Neill WW, Safian RD. Perforations after percutaneous coronary interventions: clinical, angiographic, and therapeutic observations. Cathet Cardiovasc Diagn. 1994. 32:206–212.15. Gruberg L, Pinnow E, Flood R, et al. Incidence, management and outcome of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol. 2000. 86:680–682.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Immediate Stent Fracture after Zotarolimus-Eluting Stent Implantation
- Late Stent Thrombosis Associated with Late Stent Malapposition after Drug-Eluting Stenting: A Case Report
- A Case of Extremely Very Late Stent Thrombosis 8 Years after Implantation of Drug-Eluting Stent Observed by Intravascular Ultrasound
- Drug-Eluting Stent Used to Treat a Case of Recurrent Right Coronary Artery In-Stent Restenoses often Accompanied by Acute Inferior Wall Myocardial Infarction
- Drug-Eluting Stent: Present and Future
