Progressive Manifestations of Reversible Cerebral Vasoconstriction Syndrome Presenting with Subarachnoid Hemorrhage, Intracerebral Hemorrhage, and Cerebral Infarction
- Affiliations
-
- 1Department of Neurosurgery, Hanyang University Medical Center, Seoul, Korea. hjyi8499@hanyang.ac.kr
- KMID: 2018101
- DOI: http://doi.org/10.3340/jkns.2014.56.5.419
Abstract
- Reversible cerebral vasoconstriction syndrome (RCVS) is characterized by sudden-onset headache with focal neurologic deficit and prolonged but reversible multifocal narrowing of the distal cerebral arteries. Stroke, either hemorrhagic or ischemic, is a relatively frequent presentation in RCVS, but progressive manifestations of subarachnoid hemorrhage, intracerebral hemorrhage, cerebral infarction in a patient is seldom described. We report a rare case of a 56-year-old woman with reversible cerebral vasoconstriction syndrome consecutively presenting as cortical subarachnoid hemorrhage, intracerebral hemorrhage, and cerebral infarction. When she complained of severe headache with subtle cortical subarachnoid hemorrhage, her angiography was non-specific. But, computed tomographic angiography showed typical angiographic features of this syndrome after four days. Day 12, she suffered mental deterioration and hemiplegia due to contralateral intracerebral hematoma, and she was surgically treated. For recurrent attacks of headache, medical management with calcium channel blockers has been instituted. Normalized angiographic features were documented after 8 weeks. Reversible cerebral vasoconstriction syndrome should be considered as differential diagnosis of non-aneurysmal subarachnoid hemorrhage, and repeated angiography is recommended for the diagnosis of this under-recognized syndrome.
Keyword
MeSH Terms
Figure
-
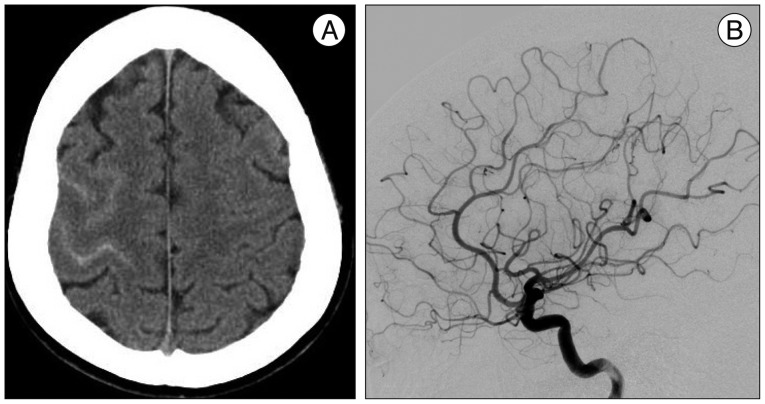
Fig. 1 A : Initial head CT scan shows subtle cortical subarachnoid hemorrhage overlying the right high frontal convexity. B : Digital subtraction angiography shows no aneurysms or arteriovenous malformation or other arterial caliber change.
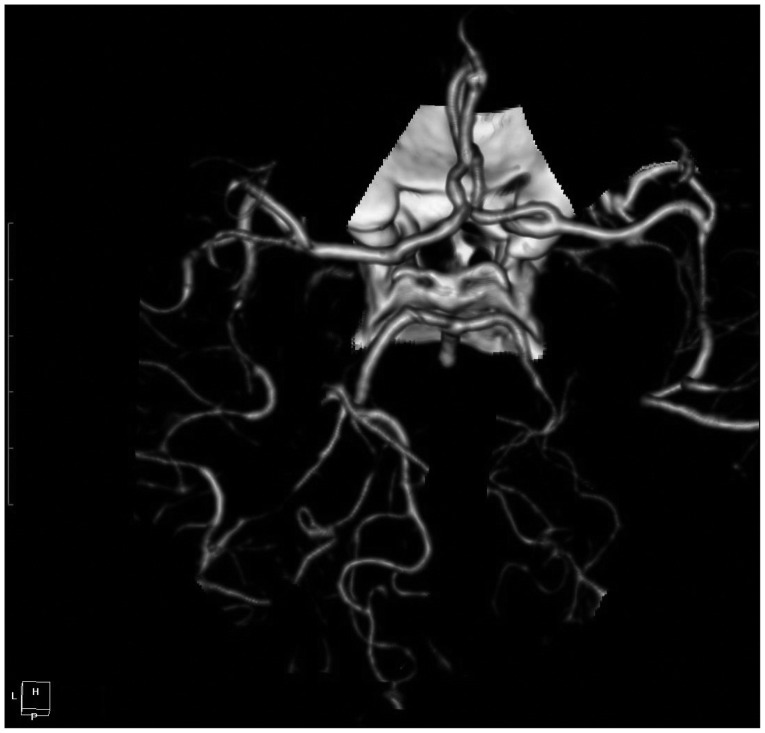
Fig. 2 Repeated CT angiographic images after 4 days on admission demonstrate prominent multifocal segmental vasoconstrictions involving superior division of both middle cerebral arteries (M2 tracts) and right posterior cerebral artery (P2 tract).
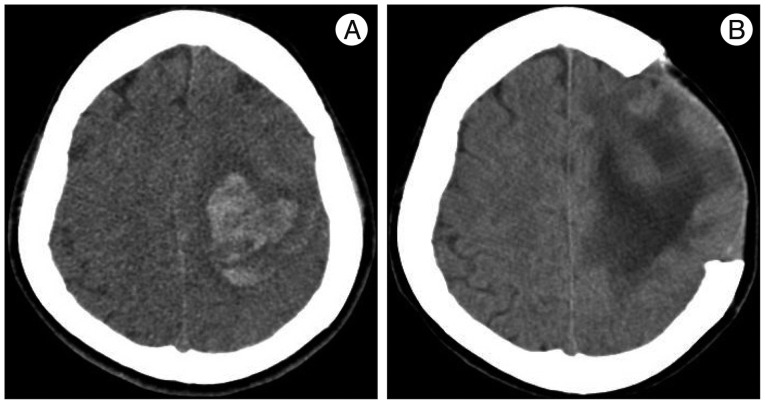
Fig. 3 A : Non-enhanced head CT at day 12 after admission shows intracerebral hemorrhage with edema on left cerebral hemisphere, associated with neurologic deterioration of the patient. B : On postoperative 12th day, CT scan reveals decreased extent of edema and hemorrhage.
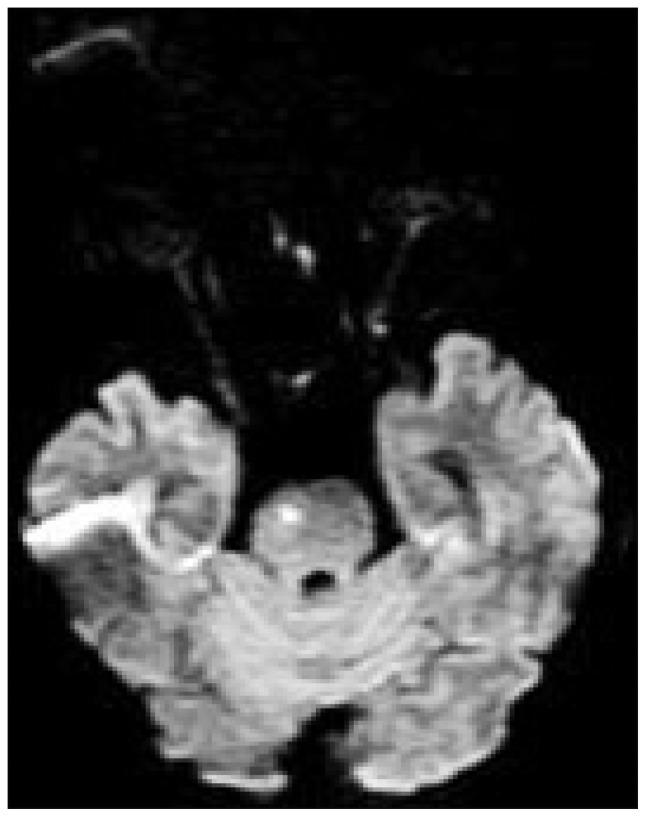
Fig. 4 The MR diffusion-weighted image on day 37 shows a hyperintense signal in the pons, suggestive of acute or subacute infarction.
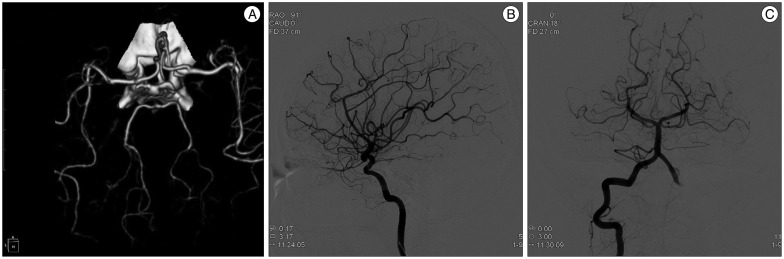
Fig. 5 Images of CT angiography (A) at 6 weeks and digital subtraction angiography (B and C) at 8weeks after initial hemorrhage demonstrate near complete resolution of segmental vasoconstriction previously seen in the both middle cerebral arteries and right posterior cerebral artery, respectively.
Reference
-
1. Ansari SA, Rath TJ, Gandhi D. Reversible cerebral vasoconstriction syndromes presenting with subarachnoid hemorrhage : a case series. J Neurointerv Surg. 2011; 3:272–278. PMID: 21990840.
Article2. Bouchard M, Verreault S, Gariépy JL, Dupré N. Intra-arterial milrinone for reversible cerebral vasoconstriction syndrome. Headache. 2009; 49:142–145. PMID: 18647181.
Article3. Calabrese LH, Dodick DW, Schwedt TJ, Singhal AB. Narrative review : reversible cerebral vasoconstriction syndromes. Ann Intern Med. 2007; 146:34–44. PMID: 17200220.
Article4. Calabrese LH, Gragg LA, Furlan AJ. Benign angiopathy : a distinct subset of angiographically defined primary angiitis of the central nervous system. J Rheumatol. 1993; 20:2046–2050. PMID: 8014931.5. Call GK, Fleming MC, Sealfon S, Levine H, Kistler JP, Fisher CM. Reversible cerebral segmental vasoconstriction. Stroke. 1988; 19:1159–1170. PMID: 3046073.
Article6. Chen SP, Fuh JL, Lirng JF, Chang FC, Wang SJ. Recurrent primary thunderclap headache and benign CNS angiopathy : spectra of the same disorder. Neurology. 2006; 67:2164–2169. PMID: 17190937.
Article7. Ducros A, Fiedler U, Porcher R, Boukobza M, Stapf C, Bousser MG. Hemorrhagic manifestations of reversible cerebral vasoconstriction syndrome : frequency, features, and risk factors. Stroke. 2010; 41:2505–2511. PMID: 20884871.
Article8. Elstner M, Linn J, Müller-Schunk S, Straube A. Reversible cerebral vasoconstriction syndrome : a complicated clinical course treated with intra-arterial application of nimodipine. Cephalalgia. 2009; 29:677–682. PMID: 19239677.
Article9. Hajj-Ali RA, Furlan A, Abou-Chebel A, Calabrese LH. Benign angiopathy of the central nervous system : cohort of 16 patients with clinical course and long-term followup. Arthritis Rheum. 2002; 47:662–669. PMID: 12522842.
Article10. Hantson P, Forget P. Reversible cerebral vasospasm, multilobular intracerebral hemorrhages, and nonaneurysmal subarachnoid hemorrhage : review of possible interrelationships. Curr Pain Headache Rep. 2010; 14:228–232. PMID: 20425193.
Article11. Moskowitz SI, Calabrese LH, Weil RJ. Benign angiopathy of the central nervous system presenting with intracerebral hemorrhage. Surg Neurol. 2007; 67:522–527. discussion 527-528. PMID: 17445624.
Article12. Nadeau SE. Diagnostic approach to central and peripheral nervous system vasculitis. Neurol Clin. 1997; 15:759–777. PMID: 9367963.
Article13. Noskin O, Jafarimojarrad E, Libman RB, Nelson JL. Diffuse cerebral vasoconstriction (Call-Fleming syndrome) and stroke associated with antidepressants. Neurology. 2006; 67:159–160. PMID: 16832100.
Article14. Quartuccio L, Tuniz F, Petralia B, Zanotti B, Skrap M, Vita SD. Delayed positivization of cerebral angiography in reversible cerebral vasoconstriction syndrome (RCVS) presenting with recurrent subarachnoid haemorrhage. Open Rheumatol J. 2012; 6:175–179. PMID: 22870164.
Article15. Refai D, Botros JA, Strom RG, Derdeyn CP, Sharma A, Zipfel GJ. Spontaneous isolated convexity subarachnoid hemorrhage : presentation, radiological findings, differential diagnosis, and clinical course. J Neurosurg. 2008; 109:1034–1041. PMID: 19035716.
Article16. Shah AK. Non-aneurysmal primary subarachnoid hemorrhage in pregnancy-induced hypertension and eclampsia. Neurology. 2003; 61:117–120. PMID: 12847171.
Article17. Singhal AB, Hajj-Ali RA, Topcuoglu MA, Fok J, Bena J, Yang D, et al. Reversible cerebral vasoconstriction syndromes : analysis of 139 cases. Arch Neurol. 2011; 68:1005–1012. PMID: 21482916.18. Spitzer C, Mull M, Rohde V, Kosinski CM. Non-traumatic cortical subarachnoid haemorrhage : diagnostic work-up and aetiological background. Neuroradiology. 2005; 47:525–531. PMID: 15971064.
Article19. Sturm JW, Macdonell RA. Recurrent thunderclap headache associated with reversible intracerebral vasospasm causing stroke. Cephalalgia. 2000; 20:132–135. PMID: 10961771.
Article20. van Gijn J, Rinkel GJ. Subarachnoid haemorrhage : diagnosis, causes and management. Brain. 2001; 124(Pt 2):249–278. PMID: 11157554.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report Reversible Cerebral Vasoconstriction Syndrome with Thunderclap Headache During Swimming
- Reversible Cerebral Vasoconstriction Syndrome and Posterior Reversible Encephalopathy Syndrome Presenting with Deep Intracerebral Hemorrhage in Young Women
- Cyclophosphamide-Associated Reversible Cerebral Vasoconstriction Syndrome Presenting as Concurrent Cerebral Infarction and Subarachnoid Hemorrhage
- Bilateral Anterior Cerebral Artery Infarction Associated with Reversible Cerebral Vasoconstriction Syndrome
- Microscopic Polyangiitis Presenting with Intracerebral Hemorrhage and Cerebral Infarction
