Clinical Significance of Radiological Stability in Reconstructed Thoracic and Lumbar Spine Following Vertebral Body Resection
- Affiliations
-
- 1Department of Neurosurgery, Korea Cancer Center Hospital, Korea Institute of Radiological and Medical Sciences, Seoul, Korea. cuk@kcch.re.kr
- KMID: 2018083
- DOI: http://doi.org/10.3340/jkns.2014.56.4.323
Abstract
OBJECTIVE
Vertebral body replacement following corpectomy in thoracic or lumbar spine is performed with titanium mesh cage (TMC) containing any grafts. Radiological changes often occur on follow-up. This study investigated the relationship between the radiological stability and clinical symptoms.
METHODS
The subjects of this study were 28 patients who underwent corpectomy on the thoracic or lumbar spine. Their medical records and radiological data were retrospectively analyzed. There were 23 cases of tumor, 2 cases of trauma, and 3 cases of infection. During operation, spinal reconstruction was done with TMC and additional screw fixation. We measured TMC settlement in sagittal plane and spinal angular change in coronal and sagittal plane at postoperative one month and last follow-up. Pain score was also checked. We investigated the correlation between radiologic change and pain status. Whether factors, such as the kind of graft material, surgical approach, and fusion can affect the radiological stability or not was analyzed as well.
RESULTS
Mean follow-up was 23.6 months. During follow-up, 2.08+/-1.65degrees and 6.96+/-2.08degrees of angular change was observed in coronal and sagittal plane, respectively. A mean of cage settlement was 4.02+/-2.83 mm. Pain aggravation was observed in 4 cases. However, no significant relationship was found between spinal angular change and pain status (p=0.518, 0.458). Cage settlement was seen not to be related with pain status, either (p=0.644). No factors were found to affect the radiological stability.
CONCLUSION
TMC settlement and spinal angular change were often observed in reconstructed spine. However, these changes did not always cause postoperative axial pain.
Keyword
MeSH Terms
Figure
-
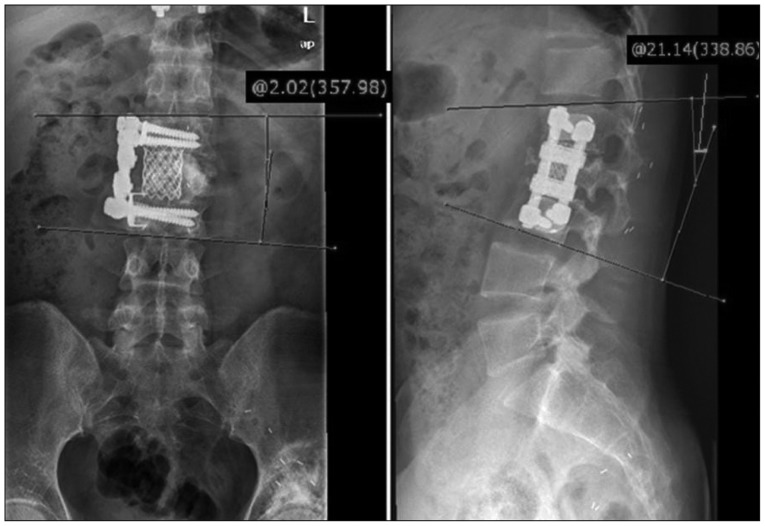
Fig. 1 Cobb's angle is measured between the superior end plate of upper vertebrae (cranial to the corpectomy site) and the inferior end plate of the lower vertebrae (caudal to corpectomy site) in coronal and sagittal plane.
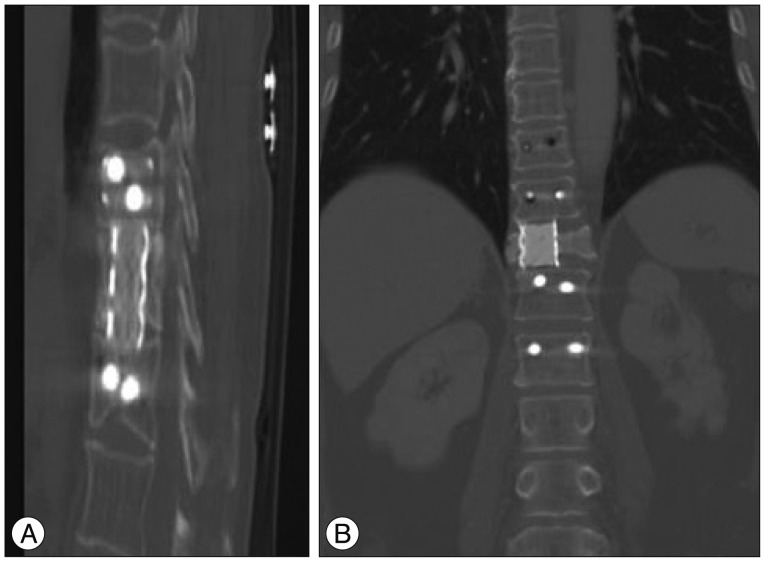
Fig. 2 A : Example of definite fusion; grade 1 by Bridwell grading system. Bone remodeling and trabeculae are seen between cage and adjacent vertebral bodies. B : Example of non-fusion; grade 3 by Bridwell grading system. Radiolucency is observed between cage and lower endplate of upper vertebral body.
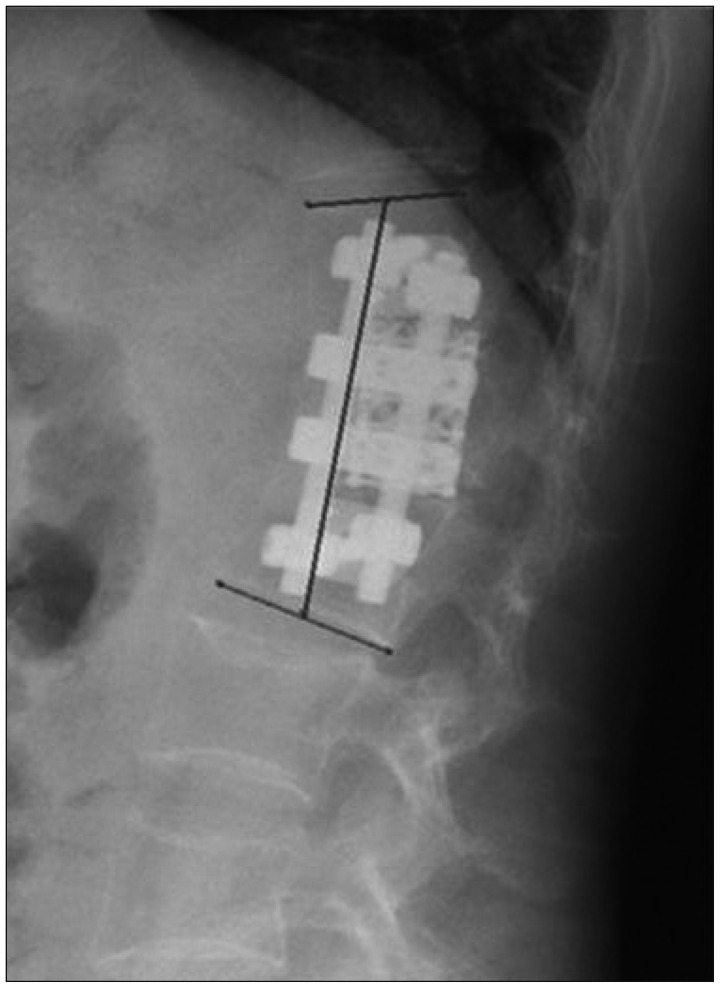
Fig. 3 Method of measuring vertebral height in fused segment. Vertebral body height is checked by measuring the distance between the midpoint of superior endplate of the upper vertebrae (the one cranial to the corpectomy site) and the midpoint of inferior endplate of the lower vertebrae (caudal to corpectomy site).

Fig. 4 A case of cage migration. After T2 corpectomy, reconstruction is done with bone cement-filled TMC and tranpedicular screw fixation. Follow-up image showed cage migration, but no aggravation of pain is observed on 47 months follow-up (case 16). TMC : titanium mesh cage.
Reference
-
1. Bagby GW. Arthrodesis by the distraction-compression method using a stainless steel implant. Orthopedics. 1988; 11:931–934. PMID: 3387340.
Article2. Bhat AL, Lowery GL, Sei A. The use of titanium surgical mesh-bone graft composite in the anterior thoracic or lumbar spine after complete or partial corpectomy. Eur Spine J. 1999; 8:304–309. PMID: 10483833.
Article3. Bridwell KH, Lenke LG, McEnery KW, Baldus C, Blanke K. Anterior fresh frozen structural allografts in the thoracic and lumbar spine. Do they work if combined with posterior fusion and instrumentation in adult patients with kyphosis or anterior column defects? Spine (Phila Pa 1976). 1995; 20:1410–1418. PMID: 7676341.
Article4. Buttermann GR, Glazer PA, Bradford DS. The use of bone allografts in the spine. Clin Orthop Relat Res. 1996; (324):75–85. PMID: 8595780.
Article5. Chen Y, Chen D, Guo Y, Wang X, Lu X, He Z, et al. Subsidence of titanium mesh cage : a study based on 300 cases. J Spinal Disord Tech. 2008; 21:489–492. PMID: 18836360.6. Dvorak MF, Kwon BK, Fisher CG, Eiserloh HL 3rd, Boyd M, Wing PC. Effectiveness of titanium mesh cylindrical cages in anterior column reconstruction after thoracic and lumbar vertebral body resection. Spine (Phila Pa 1976). 2003; 28:902–908. PMID: 12942006.
Article7. Eck KR, Bridwell KH, Ungacta FF, Lapp MA, Lenke LG, Riew KD. Mesh cages for spinal deformity in adults. Clin Orthop Relat Res. 2002; (394):92–97. PMID: 11795756.
Article8. Eck KR, Lenke LG, Bridwell KH, Gilula LA, Lashgari CJ, Riew KD. Radiographic assessment of anterior titanium mesh cages. J Spinal Disord. 2000; 13:501–509. discussion 510. PMID: 11132981.
Article9. Gokaslan ZL, York JE, Walsh GL, McCutcheon IE, Lang FF, Putnam JB Jr, et al. Transthoracic vertebrectomy for metastatic spinal tumors. J Neurosurg. 1998; 89:599–609. PMID: 9761054.
Article10. Hee HT, Majd ME, Holt RT, Pienkowski D. Better treatment of vertebral osteomyelitis using posterior stabilization and titanium mesh cages. J Spinal Disord Tech. 2002; 15:149–156. discussion 156. PMID: 11927825.
Article11. Hughes SS, Pringle T, Phillips F, Emery S. Settling of fibula strut grafts following multilevel anterior cervical corpectomy : a radiographic evaluation. Spine (Phila Pa 1976). 2006; 31:1911–1915. PMID: 16924207.
Article12. Karaeminogullari O, Tezer M, Ozturk C, Bilen FE, Talu U, Hamzaoglu A. Radiological analysis of titanium mesh cages used after corpectomy in the thoracic and lumbar spine : minimum 3 years' follow-up. Acta Orthop Belg. 2005; 71:726–731. PMID: 16459866.13. Liu JK, Rosenberg WS, Schmidt MH. Titanium cage-assisted polymethylmethacrylate reconstruction for cervical spinal metastasis : technical note. Neurosurgery. (1):Suppl. 2005; 56:E207. discussion E207. PMID: 15799818.14. Molinari RW, Bridwell KH, Klepps SJ, Baldus C. Minimum 5-year follow-up of anterior column structural allografts in the thoracic and lumbar spine. Spine (Phila Pa 1976). 1999; 24:967–972. PMID: 10332786.
Article15. Nakase H, Park YS, Kimura H, Sakaki T, Morimoto T. Complications and long-term follow-up results in titanium mesh cage reconstruction after cervical corpectomy. J Spinal Disord Tech. 2006; 19:353–357. PMID: 16826008.
Article16. Rajpal S, Hwang R, Mroz T, Steinmetz MP. Comparing vertebral body reconstruction implants for the treatment of thoracic and lumbar metastatic spinal tumors : a consecutive case series of 37 patients. J Spinal Disord Tech. 2012; 25:85–91. PMID: 22454183.
Article17. Robertson PA, Rawlinson HJ, Hadlow AT. Radiologic stability of titanium mesh cages for anterior spinal reconstruction following thoracolumbar corpectomy. J Spinal Disord Tech. 2004; 17:44–52. PMID: 14734976.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anatomy and Physiology of Lumbar Spine
- A Study on the Vertebral Body and Intervertebral Disk Indices of the Normal Korean People (A Preliminary Report)
- A study of radiographic estimation of lumbar vertebral length of Korean newborn as a method of detection offetal maturity
- Analysis on the Risk Factors of Vertebral Body Collapse in Metastatic Spine Tumors using MRI
- Radiological manifestations of tuberculosis of the spine
