J Korean Surg Soc.
2009 Sep;77(3):177-183. 10.4174/jkss.2009.77.3.177.
The Clinical Analysis of 12 Cases of Bezoars
- Affiliations
-
- 1Department of Surgery, Myongji Hospital, Kwandong University College of Medicine, Goyang, Korea. gslji@hanmail.net
- KMID: 2004216
- DOI: http://doi.org/10.4174/jkss.2009.77.3.177
Abstract
- PURPOSE
Bezoars are the uncommon result of ingestion of poorly digestible or indigestible substances. It is defined as retained concretions of animal or vegetable material in the gastrointestinal tract. The aim of this study was to review and analyze in these cases with reviewing literature. METHODS: The medical records of 12 cases, treated between May 1999 and April 2009, were reviewed. The clinical characteristics, as well as the diagnostic evaluations and results of medical and surgical treatment, were also analyzed retrospectively. RESULTS: Of the 12 cases, 6 men and 6 women, the bezoars were in the stomach, jejunum and ileum or in both stomach and jejunum in 1, 2, 7 and 2 cases, respectively. 4 patients (33.3%) had a history of gastric or duodenal ulcer following previously received gastric surgery such as subtotal gastrectomy or truncal vagotomy with pyloroplasty. In 3 cases, the bezoars were found in operative field under the impression of intestinal obstruction due to adhesive ileus, which could not be found by preoperative radiologic evaluation. Among the 12 cases, 11 cases were successfully treated by operative and endoscopic removal, but 1 case expired due to sepsis. CONCLUSION: A bezoar occurs mainly in patients who have previously undergone a gastric operation. Surgeons should keep in mind the possibility of bezoars in patients presenting an intestinal obstruction following a past gastric operation. The principle of treatment for bezoars used to be surgery, but recently gastric bezoars are often treated by gastrofiberscopy.
Keyword
MeSH Terms
Figure
-

Fig. 1 Monthly incidence of bezoars.
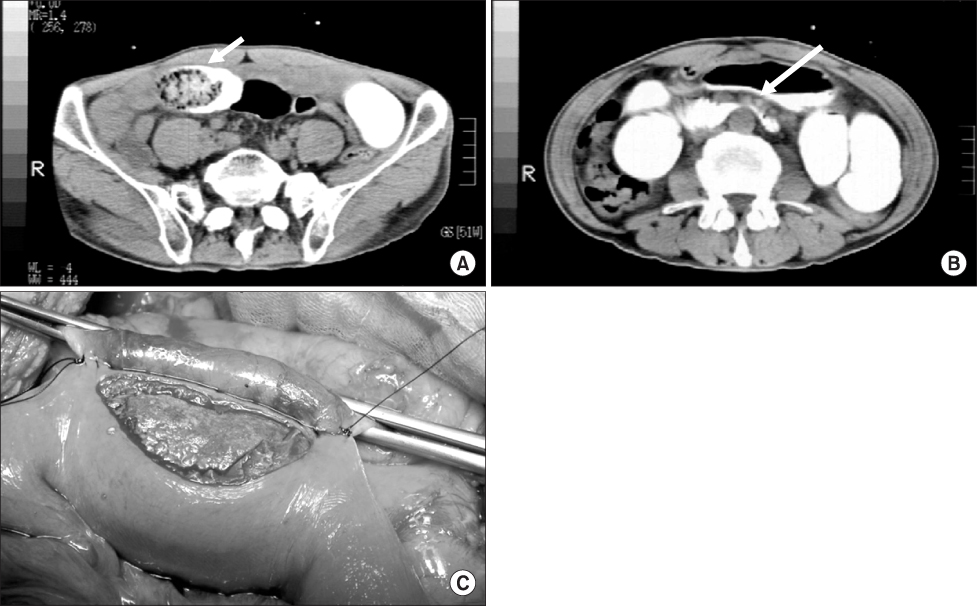
Fig. 2 The computed tomogram and operative finding of jejunal bezoar with SMA syndrome. (A) The arrow shows conglomerated jejunal phytobezoa. (B) Compressed duodenum with passage disturbance of gastrograffin by SMA. The arrow shows SMA. (C) The bezoar was removed via duodenojejunostomy.
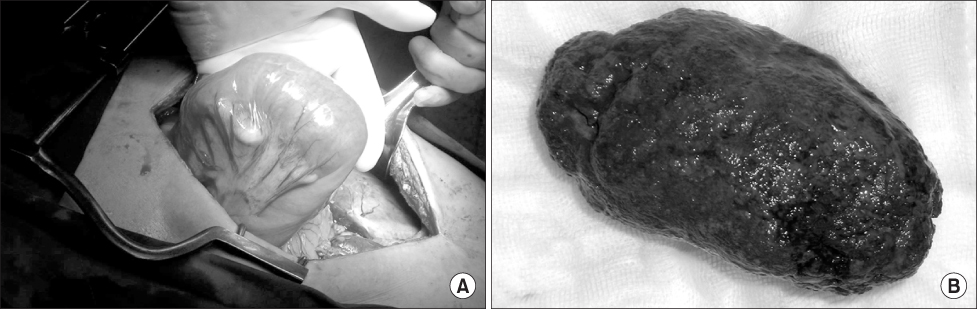
Fig. 3 The obstructive ileal phytobezoar (A) which could not be found in preoperative evaluation was identified after laparotomy extracted bezoar (B) via ileotomy.
Reference
-
1. DeBakey M, Ochsner A. Bezoars and concretions: a comprehensive review of the literature with an analysis of 303 collected cases and a presentation of 8 additional cases. Surgery. 1938. 4:934–964.2. Choi SO, Park WH, Kang JS. Gastrointestinal phytobezoars in childhood. J Korean Surg Soc. 1987. 33:186–193.3. Hong SK, Lim TJ, Park YK. A clinical study of bezoars (108 cases). Keimyung Med J. 1986. 5:68–73.4. Lee JH, Kang YW, Huh JW, Park SK, Park TW, Kang JM. Foreign bodies in the upper gastrointestinal tract: endoscopic diagnosis and removal. Korean J Gastroenterol. 1993. 25:823–827.5. Shin DK, Shin MJ, Park SH, Seong SY, Han HS, Kim KY. Nine cases of gastric bezoar removed by modified snare loop method. Korean J Gastroenterol. 1984. 16:265–268.6. Bae KS, Jeon KN, Ryeom HK. Bezoar associated with small bowel obstruction: comparison of CT and US. J Korean Radiol Soc. 2003. 48:53–58.7. Yang MJ, Ha HK, Kim JH, Sohn MJ, Kim PN, Lee MG, et al. CT imaging features of phytobezoar associated with small bowel obstruction. J Korean Radiol Soc. 2001. 44:209–215.8. Lee SG, Lee HY, Park KJ, Kim SH, Kim MC, Choi HJ, et al. The clinical analysis of 25 cases of bezoars. J Korean Surg Soc. 2005. 68:407–413.9. Min BW, Ryu JW, Kim CS, Koo BH. The clinical evaluation of the bezoars. J Korean Surg Soc. 1995. 48:133–137.10. Erzurumlu K, Malazgirt Z, Bektas A, Dervisoglu A, Polat C, Senyurek G, et al. Gastrointestinal bezoars: a retrospective analysis of 34 cases. World J Gastroenterol. 2005. 11:1813–1817.11. Chang YS, Cho CH, Whang KC. Clinical analysis of bezoars. J Korean Surg Soc. 1988. 35:445–449.12. Lee RA, Han HS, Kim OY. The intestinal obstruction due to bezoar. J Korean Surg Soc. 1999. 56:1043–1047.13. Kaplan O, Klausner JM, Lelcuk S, Skornick Y, Hammar B, Rozin R. Persimmon bezoars as a cause of intestinal obstruction: pitfalls in their surgical management. Br J Surg. 1985. 72:242–243.14. Memon SA, Mandhan P, Qureshi JN, Shairani AJ. Recurrent Rapunzel syndrome - a case report. Med Sci Monit. 2003. 9:CS92–CS94.15. Wang PY, Skarsgard ED, Baker RJ. Carpet bezoar obstruction of the small intestine. J Pediatr Surg. 1996. 31:1691–1693.16. Jeong YH, Moon TI, Rhee JK, Chae KM. Clinical analysis of 17 cases of bezoar. Korean J Gastroenterol. 1989. 21:572–576.17. Kim CM, Rhee YR. Clinical analysis of diospyrobezoars (bezoars). J Korean Surg Soc. 1983. 25:1312–1319.18. Park NK, Suh JW. The clinical observation of 20 cases of bezoars. J Korean Surg Soc. 1973. 15:425–428.19. Ripolles T, Garcia-Aguayo J, Martinez MJ, Gil P. Gastrointestinal bezoars: sonographic and CT characteristics. AJR Am J Roentgenol. 2001. 177:65–69.20. Delpre G, Glanz I, Neeman A, Avidor I, Kadish U. New therapeutic approach in postoperative phytobezoars. J Clin Gastroenterol. 1984. 6:231–237.21. Yol S, Bostanci B, Akoglu M. Laparoscopic treatment of small bowel phytobezoar obstruction. J Laparoendosc Adv Surg Tech A. 2003. 13:325–326.22. Robles R, Lujan JA, Parrilla P, Torralba JA, Escamilla C. Laparoscopic surgery in the treatment of small bowel obstruction by bezoar. Br J Surg. 1995. 82:520.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Megaduodenum with Duodenal Diospyrobezoars
- A Single-center 12-year Experience of Patients with Gastrointestinal Bezoars
- Endoscopic Removal of Efferent Loop Bezoars in Postgastretomy Pateints
- Surgical Management of Intestinal Obstruction from Phytobezoar
- Bezoar Associated with Small Bowel Obstruction: Comparison of CT and US
