Simultaneous Lung and Liver Aspergillus in a Kidney Transplant Recipient
- Affiliations
-
- 1Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea. eahwang@gmail.com
- 2Keimyung University Kidney Institute, Daegu, Korea.
- 3Department of Surgery, Keimyung University School of Medicine, Daegu, Korea.
- KMID: 2003536
- DOI: http://doi.org/10.4285/jkstn.2012.26.3.202
Abstract
- Invasive opportunistic infection by Aspergillus fungus is life-threatening for kidney transplant recipients. The occurrence of aspergillosis by hematogenous dissemination can affect multiple organs. Despite having a lower incidence rate relative to bacterial or viral infections in kidney transplant recipients, fungal infections produce the highest number of mortalities. We report a simultaneous case of invasive aspergillosis in the lung and liver of a 52-year-old female patient who underwent living donor kidney transplant. She suffered massive blood loss and high-volume transfusions due to postoperative bleeding. One month after transplantation, she reported intermittent coughing without febrile sensation. Computed tomography revealed nodules on the right and left upper lobes of the lung and multiple cystic liver lesions. Based on pathologic findings and culture from aspirate, she was diagnosed with invasive aspergillosis involving the liver and lung. After a 4 month voriconazole treatment the nodules in the lung and liver disappeared.
Keyword
MeSH Terms
Figure
-

Fig. 1 Nodular opacities were newly developed in left and right upper lung.
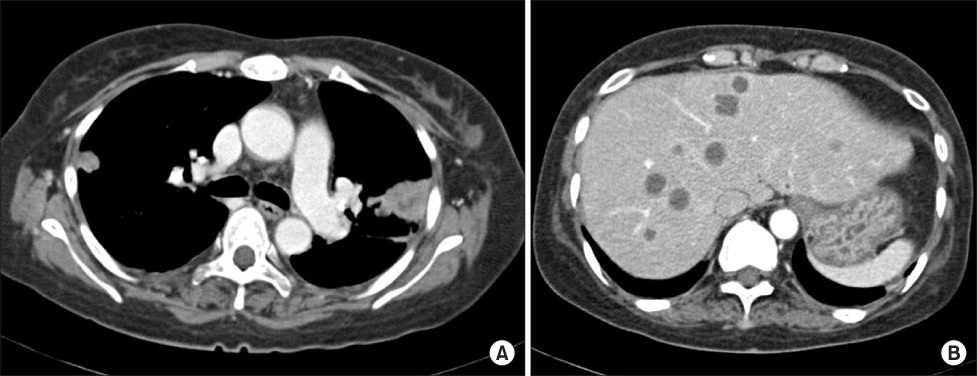
Fig. 2 (A) Chest computed tomography (CT) revealed contrast enhanced nodular consolidations in right upper lobe apical and left upper lobe apicoposterior segment. (B) Abdominal CT revealed multiple cystic lesions with enhancing wall in right and left hepatic lobes.
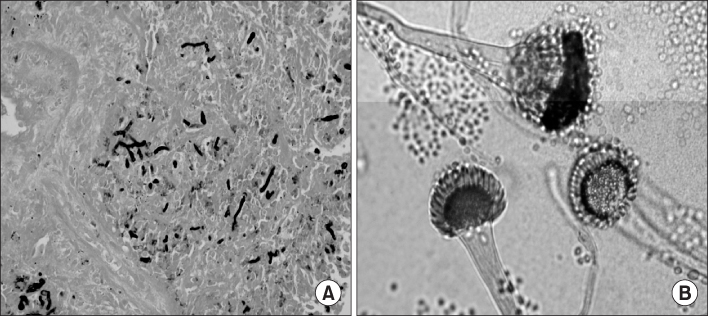
Fig. 3 (A) Lung biopsy. Many fungal organisms were identified in inflammatory and necrotic areas (Gomori-methenamine silver stain, ×400). (B) Liver aspiration. Delicate blue hyphae and fruiting structures were identified in cystic lesions (Lactophenol cotton blue stain, ×400).
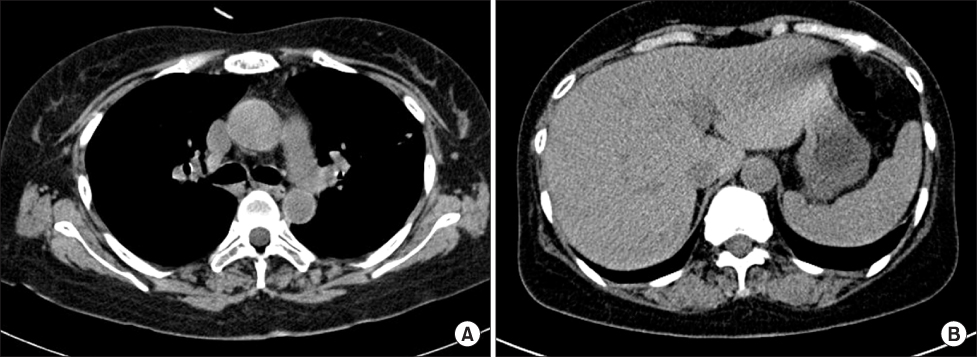
Fig. 4 Subpleural lung nodules (A) and multiple hepatic abscesses (B) were not detected after treatment with voriconazole for 4 months.
Cited by 1 articles
-
Fatal Invasive Pulmonary Aspergillosis after Combined Induction with Rituximab and Antithymocyte Globulin for Kidney Transplantation in a Sensitized Recipient, and Early Rejection Therapy with Plasmapheresis and Low-dose Immunoglobulin
Da Wun Jeong, Sang-Ho Lee, Ju-Young Moon, Yang-Gyun Kim, Yu Ho Lee, Kipyo Kim, Hochul Park, Sun Hyung Joo
J Korean Soc Transplant. 2017;31(1):52-57. doi: 10.4285/jkstn.2017.31.1.52.
Reference
-
1. Singh N, Paterson DL. Aspergillus infections in transplant recipients. Clin Microbiol Rev. 2005. 18:44–69.2. Minari A, Husni R, Avery RK, Longworth DL, DeCamp M, Bertin M, et al. The incidence of invasive aspergillosis among solid organ transplant recipients and implications for prophylaxis in lung transplants. Transpl Infect Dis. 2002. 4:195–200.
Article3. Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, Marr KA, et al. Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008. 46:327–360.
Article4. Paya CV. Fungal infections in solid-organ transplantation. Clin Infect Dis. 1993. 16:677–688.
Article5. Gavalda J, Len O, San Juan R, Aguado JM, Fortun J, Lumbreras C, et al. Risk factors for invasive aspergillosis in solid-organ transplant recipients: a case-control study. Clin Infect Dis. 2005. 41:52–59.
Article6. Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med. 2002. 347:408–415.
Article7. Marty FM, Cosimi LA, Baden LR. Breakthrough zygomycosis after voriconazole treatment in recipients of hematopoietic stem-cell transplants. N Engl J Med. 2004. 350:950–952.
Article8. Venkataramanan R, Zang S, Gayowski T, Singh N. Voriconazole inhibition of the metabolism of tacrolimus in a liver transplant recipient and in human liver microsomes. Antimicrob Agents Chemother. 2002. 46:3091–3093.
Article9. Greene RE, Schlamm HT, Oestmann JW, Stark P, Durand C, Lortholary O, et al. Imaging findings in acute invasive pulmonary aspergillosis: clinical significance of the halo sign. Clin Infect Dis. 2007. 44:373–379.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nocardia Brain Abscess in a Liver Transplant Recipient
- Disseminated aspergillosis with cutaneous aspergillosis and aspergergillus thyroiditis in a renal allograft recipient
- Simultaneous Liver, Kidney Transplantation: A Single Center Experience
- Fusarium infection in a lung transplant patient and a simultaneous heart-kidney transplant patient
- High success rate of liver and kidney transplant during seven months COVID-19 period
