The Rectal Fistula Complicating an L5-S1 Postoperative Spondylodiscitis: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Kyung Hee University School of Medicine, Seoul, Korea.
- 2Department of Surgery, Kyung Hee University School of Medicine, Seoul, Korea.
- 3Department of Orthopedic Surgery, Chunchon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea. seo-em@hanmail.net
- KMID: 2003118
- DOI: http://doi.org/10.4184/jkss.2009.16.3.222
Abstract
- To our knowledge, there are no reported cases of rectal fistula complicating spondylodiscitis. We report the first case of a rectal fistula communicating with the site of postoperative recurrent spondylodiscitis. A-59-year-old female had recurrent spondylodiscitis after an open discectomy for L5-S1 eight years earlier. She underwent three operations including two anterior lumbar interbody fusion procedures after an open discectomy. Radiographic studies revealed severe bony destruction with abscess collection within the L5-S1 intervertebral disc space with fistula formation into the rectum. The fistula was confirmed by a Barium enema colon study and sigmoidscopy. The patient underwent a staged operation consisting of a rectosigmoid colon resection, anterior interbody fusion and posterior instrumented fusion. Rectum related complications were suspected in this case of recurrent spondylodiscitis.
Keyword
MeSH Terms
Figure
-
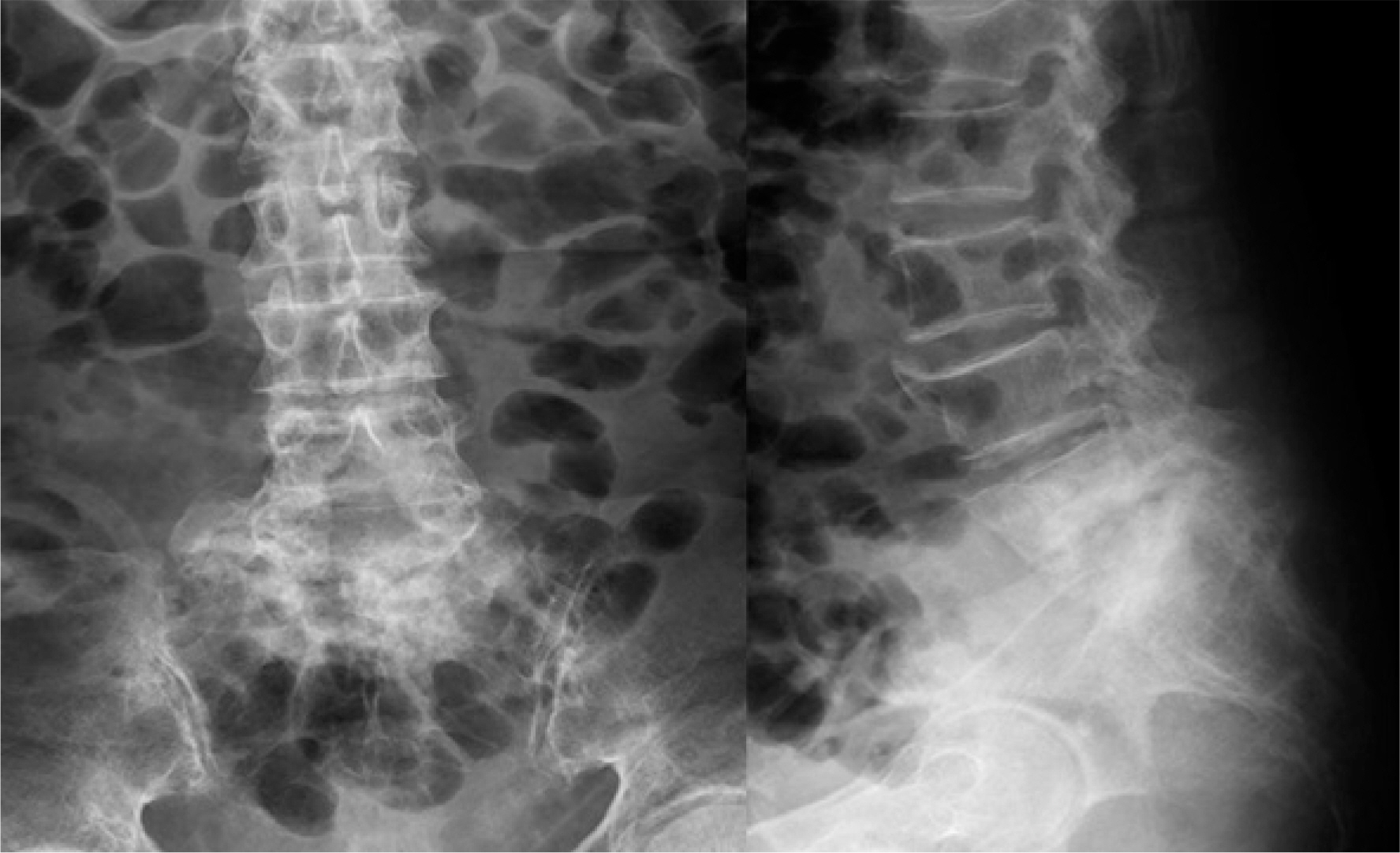
Fig. 1. Plain radiographs of the lumbar spine showing a narrowed disc space at L5-S1 with endplate destruction, reactive sclerosis of the vertebral bodies.
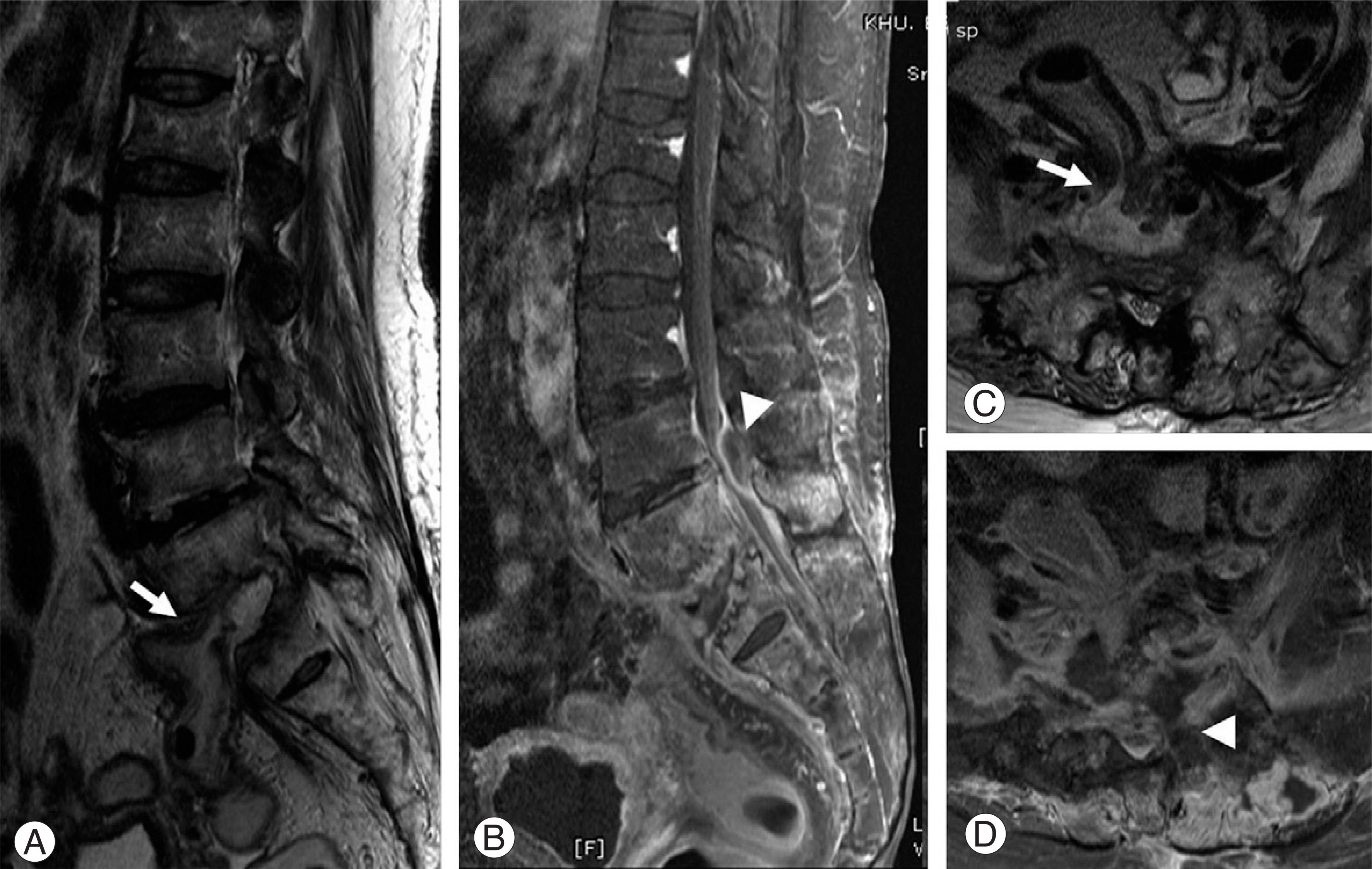
Fig. 2. (A, C) T2-weighted and (B, D) T1-weighted contrast enhanced MR sagittal images showing an abscess in L5-S1 disc space, extending into the rectum (arrows) and the epidural space (arrow heads).
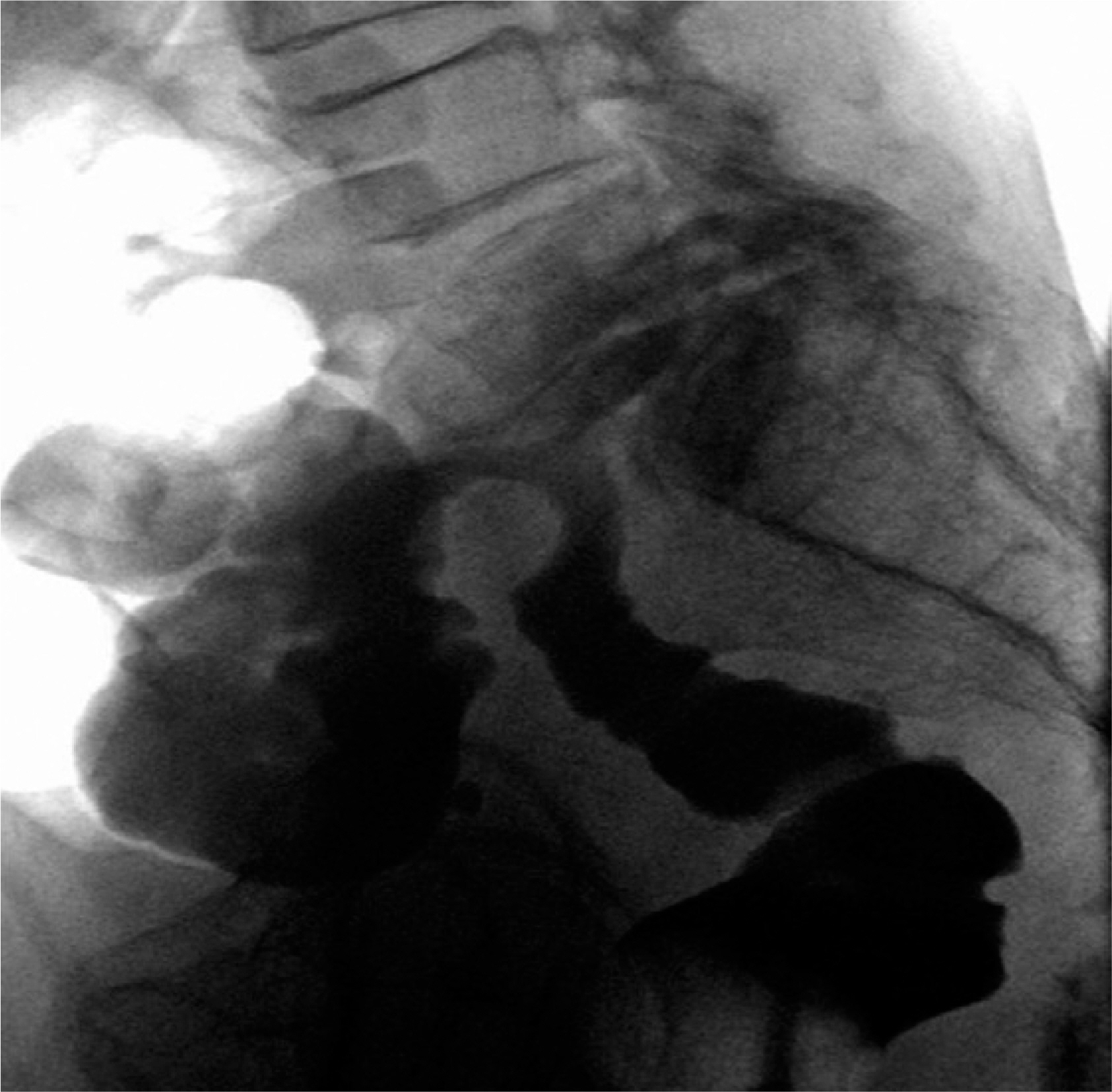
Fig. 3. Barium enema colon study showing dye leakage into L5-S1 disc space.
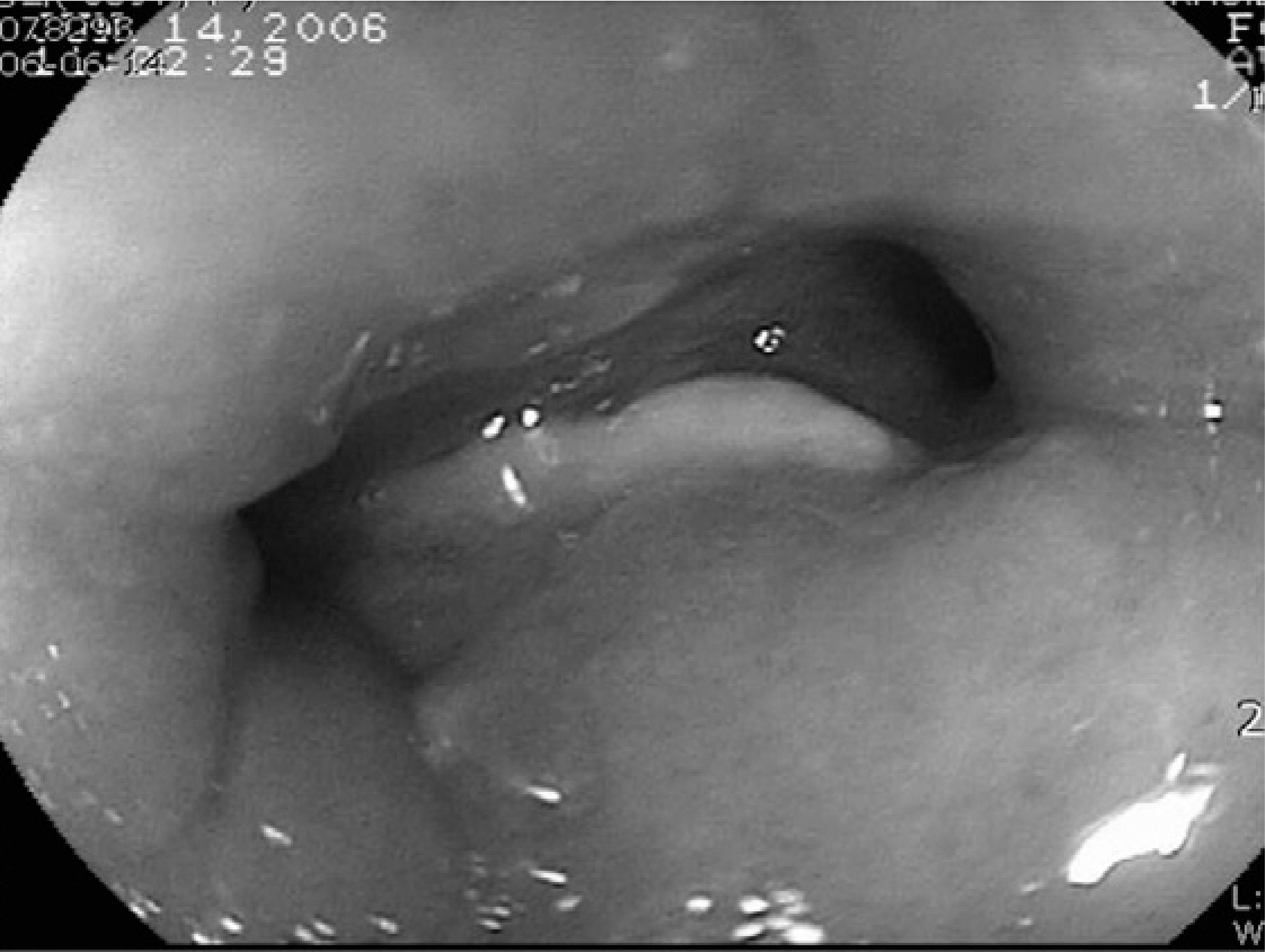
Fig. 4. Photographs showing two orifices at the 15cm upper portion from the anal verge on sigmoidscopy.
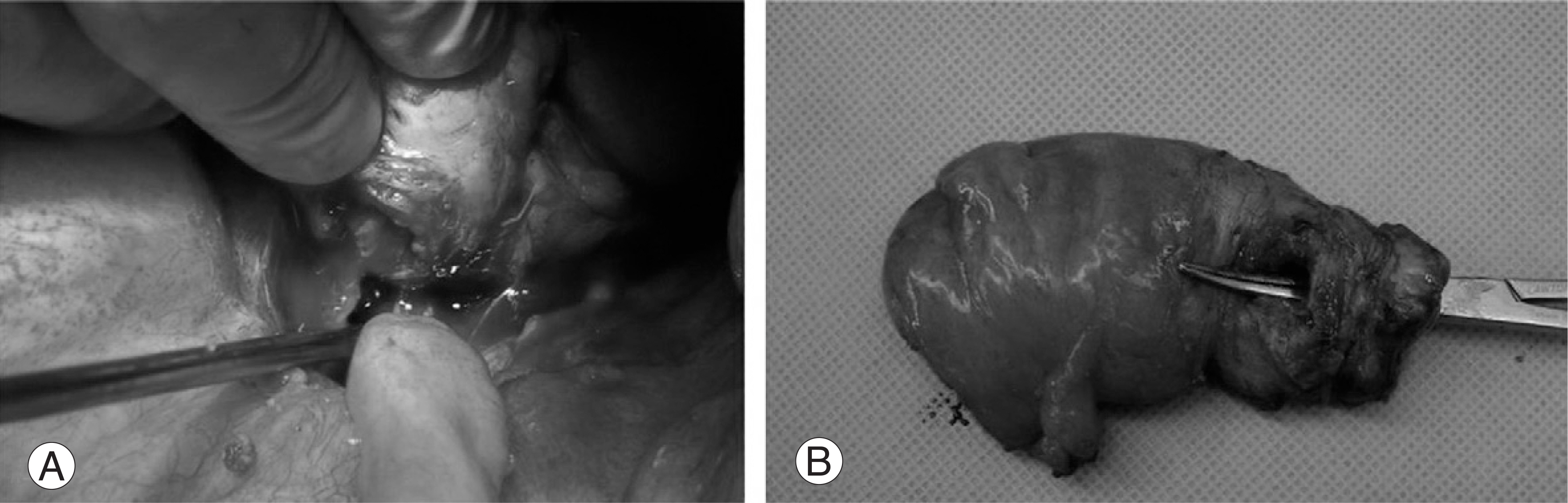
Fig. 5. Intraoperative photographs showing resection and reanastomosis procedure of the rectum (A) and rectal specimen with fistula (B).
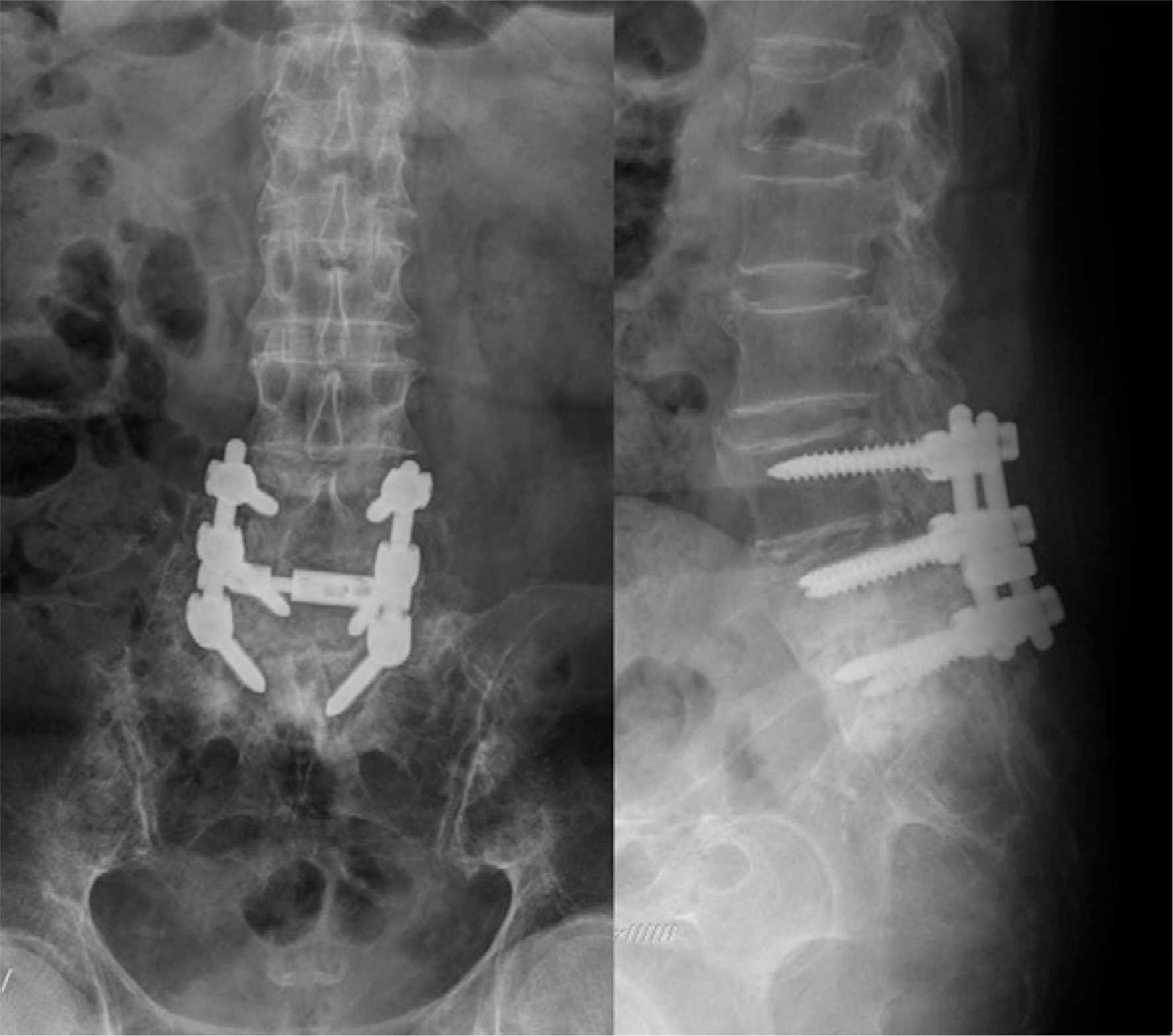
Fig. 6. Radiographs of lumbar spine showing posterior instrumentation and posterolateral fusion at L4-5-S1 vertebra to restore the mechanical integrity of the spinal motion segments.
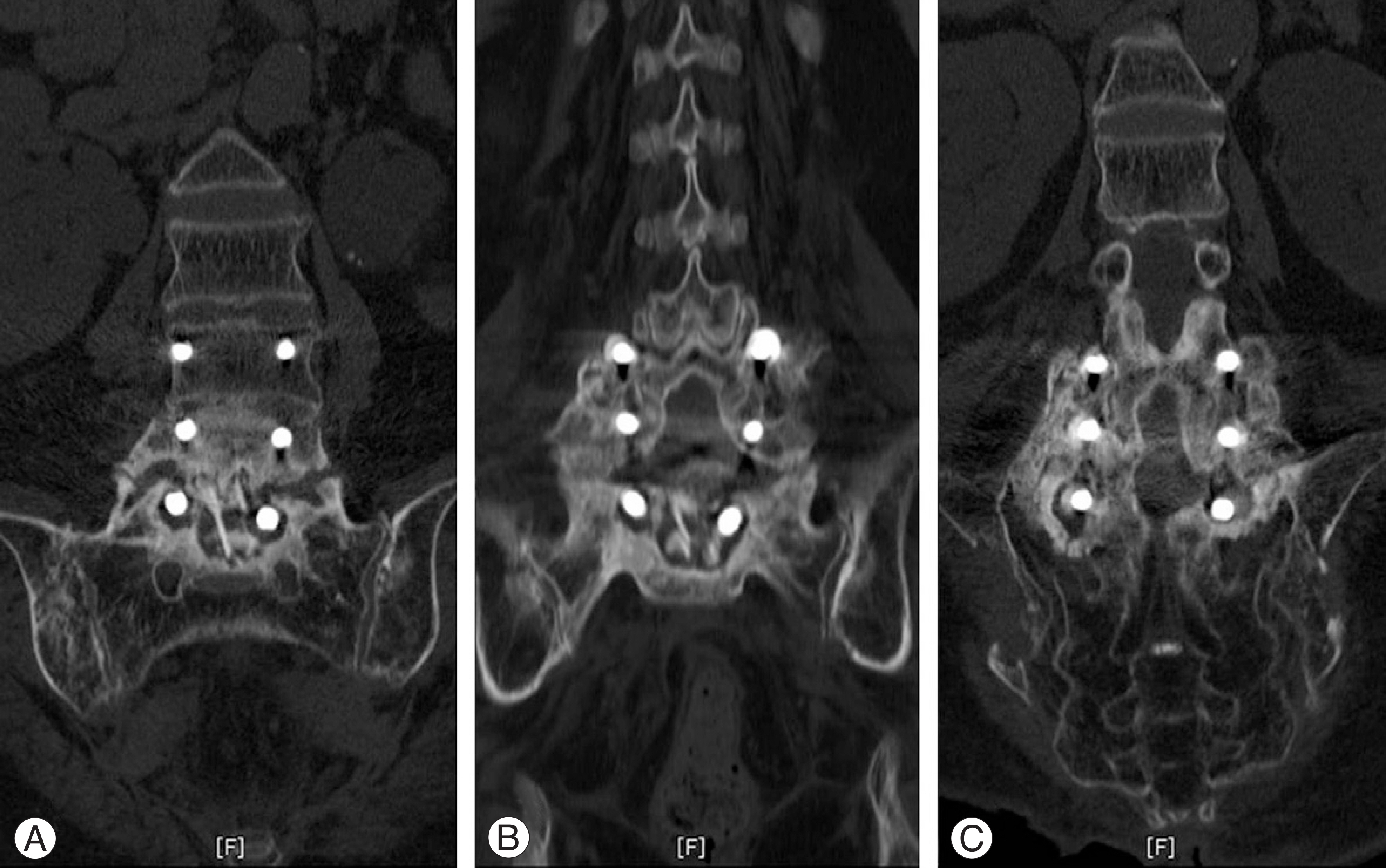
Fig. 7. CT scans showing incomplete bony union of autogenous fibula bone graft at L5-S1 (A) but bony union of L4-5-S1 posterolateral fusion (B,C).
Reference
-
1). Twyman RS, Robertson P, Thomas MG. Meningitis complicating spinal surgery. Spine. 1996; 21:763–765.
Article2). Kapoor B, Toms A, Hooper P, Fraser AM, Cox CW. Infective lumbar discitis following laparoscopic sacro-colpopexy. J R Coll Surg Edinb. 2002; 24:709–710.3). Schulze CJ, Mayer HM. Exogenous lumbar spondylodici-tis following a stabwound injury and vertebral fracture. A case report and review of literature. Eur Spine J. 1995; 4:357–359.4). Gottwald M, Andress HJ, Schinkel C. Unspecific spoondylodiscitis following anastomotic leakage after rectal resection. Zentrabli Chir. 2003; 128:337–340.5). Brown EM, Pople IK, de louvois J, et al. .:. Spine update: Prevention of postoperative infection in patient undergoing spinal surgery. Spine. 2004; 29:938–945.6). Capen DA, Calderone RR, Green A. Perioperative risk factors for wound infections after lower back fusion. Orthop Clin North Am. 1996; 27:83–86.7). Klevens RM, Edwards JR, Tenover FC, McDonald LC, Horan T, Gaynes R. Changes in the epidemiology of methicillin-resistant aureus in intensive care units in US hospitals, 1992-2003. Clin Infect Dis. 2006; 42:389–391.8). Al-Nammari SS, Lucas JD, Lam KS. Hematogenous methicillin-resistant Staphylococcus aureus spondylodiscitis. Spine. 2007; 32:2480–2486.
Article9). Stevens QE, Seibly JM, Chen YH, Dickerman RD, Noel J, Kattner KA. Reactivation of dormant lumbar methicillin-resistant Staphylococcus aureus osteomyelitis after 12 years. J Clin Neurosci. 2007; 14:585–589.
Article10). Mann S, Schu¨tze M, Sola S, Piek J. Nonspecific pyogenic spondylodiscitis: clinical manifestation, surgical treatment, and outcome in 24 patients. Neurosurg Focus. 2004; 17:3.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Polymicrobial Fungal and Bacterial Spondylodiscitis
- Candida Parapsilosis Spondylodiscitis after Lumbar Discectomy
- Radiological observation of the spondylolisthesis: The comparison between L4-L5 and L5-S1 spondylolisthesis inplain film and myelographic of finding
- Rectovaginal Fistula Complicating Stapled Hemorrhoidectomy
- Survival Rates and Risk Factors for Cephalad and L5-S1 Adjacent Segment Degeneration after L5 Floating Lumbar Fusion : A Minimum 2-Year Follow-Up
