Contrast-Enhanced Ultrasound and Computed Tomography Findings of Recurrent Ovarian Steroid Cell Tumor Presenting with Peritoneal Seeding: A Case Report
- Affiliations
-
- 1Department of Radiology, Wonkwang University School of Medicine & Hospital, Iksan, Korea. yjyh@wonkwang.ac.kr
- 2Department of Pathology, Wonkwang University School of Medicine & Hospital, Iksan, Korea.
- KMID: 2002862
- DOI: http://doi.org/10.3348/jksr.2013.69.5.399
Abstract
- We present ultrasonography and computed tomography (CT) findings of a case of recurrent ovarian steroid cell tumor presenting with peritoneal seeding in a 45-year-old woman. On abdominal ultrasonography, there were multiple hypoechoic round masses in the peritoneal cavity including the perihepatic area. Contrast-enhanced ultrasonography showed intense homogenous enhancement on the arterial phase and delayed prolonged enhancement of the masses. CT revealed multiple peritoneal solid masses with strong enhancement. Five years ago, the patient had been diagnosed with a steroid cell tumor of the left ovary. At that time, the CT showed a well-enhancing, lobulating, large solid mass at the left adnexa. Imaging findings of the peritoneal masses suggested peritoneal seeding from the preexisting ovarian steroid cell tumor. For treatment of the metastatic lesions in the perihepatic area, ultrasonography-guided radiofrequency ablation (RFA) was performed, and debulking surgery for the peritoneal masses was done. Six months later, complete ablation of the perihepatic metastases by RFA and a marked decrease in the peritoneal metastases by surgery were found on the follow-up CT.
MeSH Terms
Figure
-
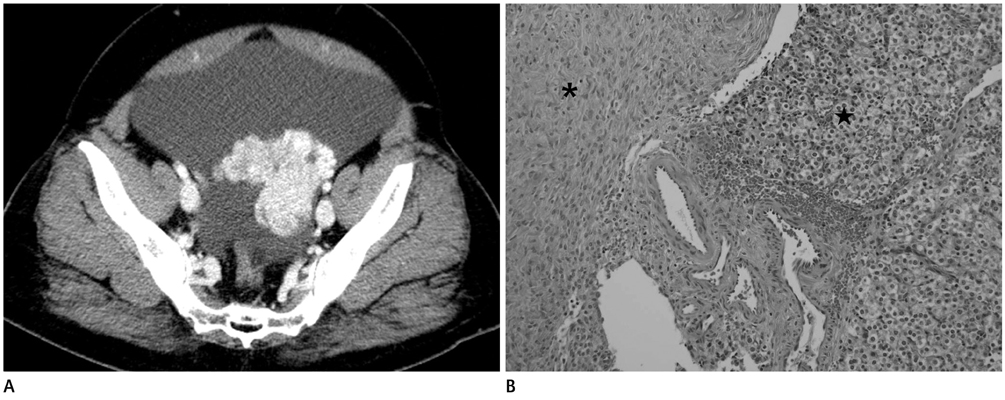
Fig. 1 Ovarian steroid cell tumor in a 45-year-old female patient. A. Initial abdominopelvic CT shows 7.7 × 6.6 cm sized well-enhancing solid mass with lobulating contour in left ovary suggesting ovarian cancer. Large amount of ascites was also noted. B. Photomicrograph of the ovarian mass (★) shows round nuclei and clear cytoplasm suggesting steroid cell tumor. Note the waving appearance of the nuclei in normal ovarian stroma (*) (hematoxylin-eosin, × 200).
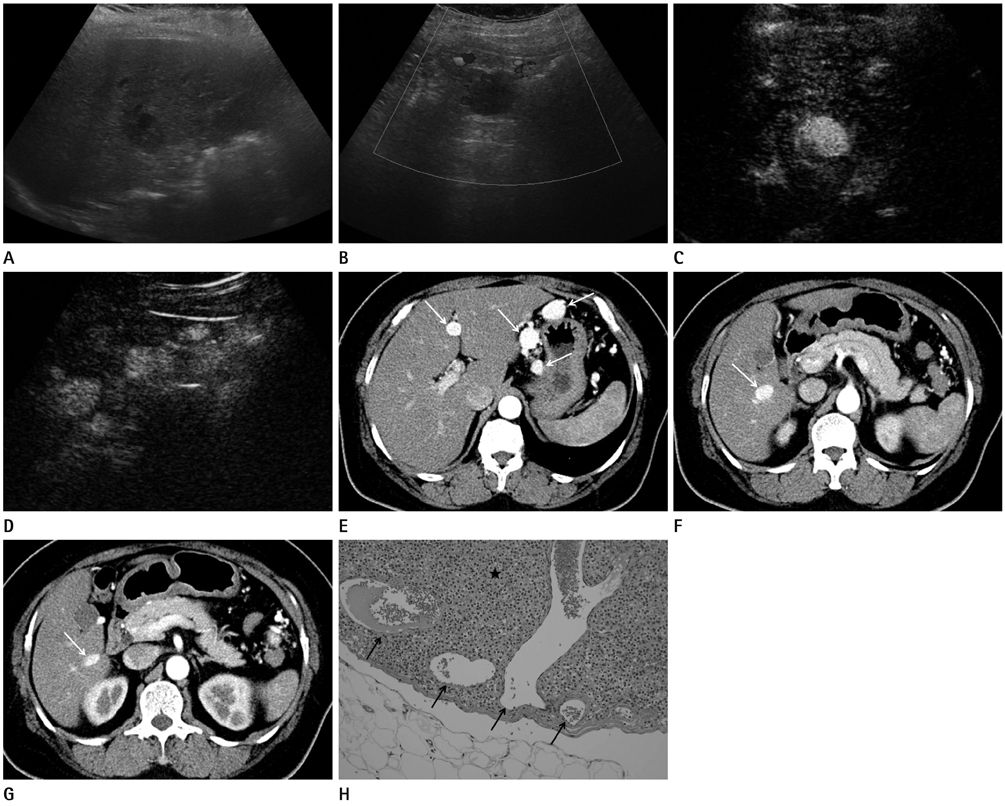
Fig. 2 Recurrent ovarian steroid cell tumor presenting peritoneal seeding after 5 years and 10 months in same patient of Fig. 1. A, B. Abdominal ultrasonography shows multiple well-defined hypoechoic masses in the liver and peritoneal cavity including 3.0 × 2.1 cm sized mass in hepatic segment 6 (A) and 1.4 × 1.3 cm sized mass in hepatic segment 3 (not shown). Color Doppler ultrasound image shows slightly increased vascular flows at peripheral portion of the masses (B). C, D. Contrast-enhanced ultrasonography shows intense homogenous enhancement of the hepatic mass on arterial phase (C) and delayed prolonged contrast enhancement of the omental masses (D). E-G. Abdominopelvic CT shows multiple well-enhancing round masses (arrows) in the peritoneum, including perigastric, gastrohepatic and hepaticoduodenal ligaments, and mesenteric areas and fissure for ligamentum teres (E). Note another well-enhancing round mass (arrow) which is thought to be existing in segment 6 of the liver (F). But, axial image adapted from F shows that the mass is an extrahepatic mass (arrow) which is grown from accessory hepatic fissure and interrupting hepatic parenchyme (G). H. Photomicrographs of the omental mass (★) shows round nuclei and clear cytoplasm suggesting metastatic steroid cell tumor from preexisting ovarian steroid tumor. Note rich vascularity (arrows) of the mass (hematoxylin-eosin, × 200).
Reference
-
1. Young RH, Shully RE. Steroid cell tumors of the ovary. In : Fox H, Wells M, editors. Obstetric & Gynecological Pathology. Spain: Churchill Livingstone;2003. p. 845–856.2. Haji AG, Sharma S, Babu M, Vijaykumar D, Chitrathara K. Androgen secreting steroid cell tumor of the ovary in a young lactating women with acute onset of severe hyperandrogenism: a case report and review of literature. J Med Case Rep. 2007; 1:182.3. Ye L, Wu XL, Xu L, Huang Q, Sun L, He Y, et al. [Ovarian steroid cell tumor, not otherwise specified: a clinicopathologic study]. Zhonghua Bing Li Xue Za Zhi. 2007; 36:516–520.4. Kim YT, Kim SW, Yoon BS, Kim SH, Kim JH, Kim JW, et al. An ovarian steroid cell tumor causing virilization and massive ascites. Yonsei Med J. 2007; 48:142–146.5. Liu AX, Sun J, Shao WQ, Jin HM, Song WQ. Steroid cell tumors, not otherwise specified (NOS), in an accessory ovary: a case report and literature review. Gynecol Oncol. 2005; 97:260–262.6. Boyraz G, Selcuk I, Yusifli Z, Usubutun A, Gunalp S. Steroid cell tumor of the ovary in an adolescent: a rare case report. Case Rep Med. 2013; 2013:527698.7. Outwater EK, Wagner BJ, Mannion C, McLarney JK, Kim B. Sex cord-stromal and steroid cell tumors of the ovary. Radiographics. 1998; 18:1523–1546.8. Al-Farsi A, Al-Talib A. Steroid cell tumor. Sultan Qaboos Univ Med J. 2008; 8:358–359.9. Jung SE, Rha SE, Lee JM, Park SY, Oh SN, Cho KS, et al. CT and MRI findings of sex cord-stromal tumor of the ovary. AJR Am J Roentgenol. 2005; 185:207–215.10. Saida T, Tanaka YO, Minami M. Steroid cell tumor of the ovary, not otherwise specified: CT and MR findings. AJR Am J Roentgenol. 2007; 188:W393–W394.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unusual Peritoneal Metastasis of Late Recurrent Uterine Cervical Cancer: A Case Report and Literature Review
- Recurrent ovarian steroid cell tumor, not otherwise specified managed with debulking surgery, radiofrequency ablation, and adjuvant chemotherapy
- Retrospective study of functional ovarian cysts on ultrasonographic findings
- An asymptomatic ovarian steroid cell tumor with complete cystic morphology: A case report
- Hematometra Due to Cervical Stenosis in a Postmenopausal Woman with Incidental Ovarian Steroid Cell Tumor: A Case Report
