Full mouth rehabilitation in a patient with loss of vertical dimension caused by severe tooth loss: a case report
- Affiliations
-
- 1Department of Prosthodontics, Hallym University Sacred Heart Hospital, Anyang, Korea. hyewonshim@hanmail.net
- KMID: 2000146
- DOI: http://doi.org/10.4047/jkap.2014.52.1.42
Abstract
- Decrease of occlusal vertical dimension (OVD) due to loss of teeth structure and destruction of the occlusal plane by severely worn dentition may cause cross bite or temporomandibular joint disorder by following change of facial feature or the loss of anterior guidance. Full mouth rehabilitation via an increase of the OVD can be considered to avoid this problem and proper evaluation of patient's OVD is essential. An 80 year old male visited for overall prosthodontic treatment, cross bite due to continuous wear and following decrease of the OVD were observed. We analyzed the existing occlusal relationship using the diagnostic cast, the radiographic evaluation and clinical test, and then proper increase of OVD was selected. The new OVD on diagnostic wax up was placed by the temporary restoration. After 3 months of observation period, final restoration with fixed partial dentures and implant overdenture were made. Throughout the follow-up period of 8 months, the aesthetic and functional improvement can be obtained.
MeSH Terms
Figure
-

Fig. 1. Intraoral photographs. A: Right lateral view, B: Frontal view, C: Left lateral view, D: Maxillary occlusal view, E: Mandibular occlusal view.

Fig. 2. Panoramic radiograph before treatment.

Fig. 3. TMJ series. A: Right view on opened state, B: Right view on closed state, C: Left view on opened state, D: Left view on closed state.
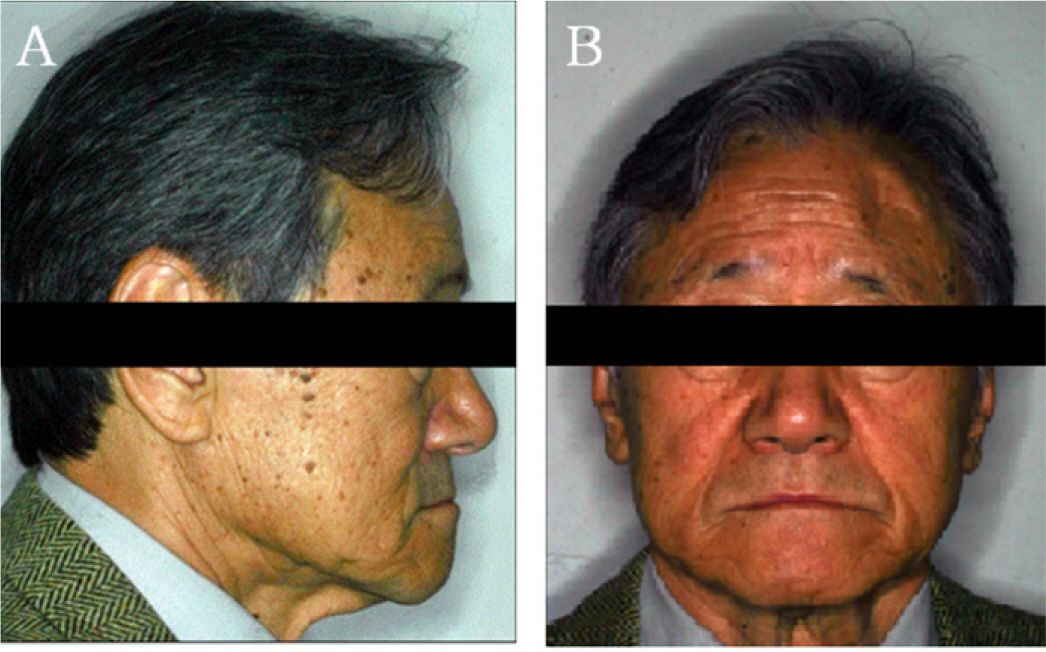
Fig. 4. Facial photographs before treatment. A: Lateral view, B: Frontal view.

Fig. 5. Vertical dimension evaluation. A: Vertical dimension at the centric occlusion, B: Vertical dimension at physical rest position. The interocclusal distance is the difference between A and B.

Fig. 6. Model analysis. A: Mounted diagnostic model with old occlusal vertical dimension on centric relationship, B: Diagnostic wax up model with new occlusal vertical dimension.

Fig. 7. Provisional restoration. A: First provisional restoration, B: Second provisional restoration after mandibular residual anterior teeth extraction.

Fig. 8. Final restoration. A: Frontal view, B: Maxillary occlusal view, C and D: Mandibular occlusal view, E: Panoramic radiographs after treatment.
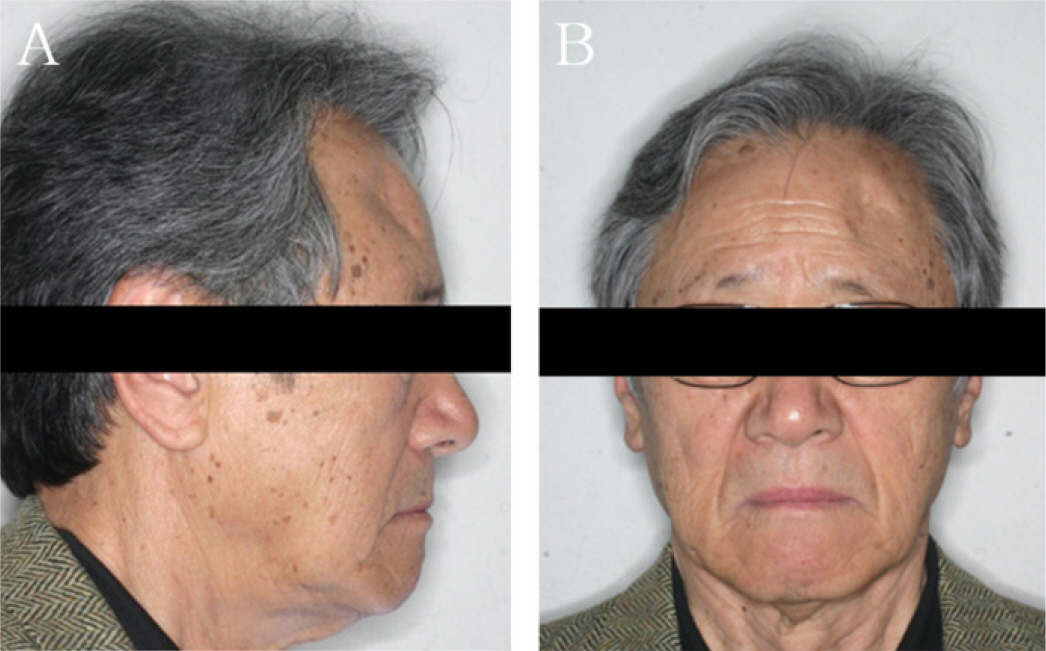
Fig. 9. Facial photographs after treatment. A: Lateral view B. Frontal view.
Reference
-
1.Rivera-Morales WC., Mohl ND. Relationship of occlusal vertical dimension to the health of the masticatory system. J Prosthet Dent. 1991. 65:547–53.
Article2.Abduo J. Safety of increasing vertical dimension of occlusion: a systematic review. Quintessence Int. 2012. 43:369–80.3.Bloom DR., Padayachy JN. Increasing occlusal vertical dimension-why, when and how. Br Dent J. 2006. 200:251–6.4.Abduo J., Lyons K. Clinical considerations for increasing occlusal vertical dimension: a review. Aust Dent J. 2012. 57:2–10.
Article5.Murphy T. Compensatory mechanisms in facial height adjustment to functional tooth attrition. Aust Dent J. 1959. 4:312–23.
Article6.Hemmings KW., Darbar UR., Vaughan S. Tooth wear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent. 2000. 83:287–93.
Article7.Dawson PE. Functional occlusion: from TMJ to smile design. St. Louis; Mo: Mosby;2007. p. 430–52.8.Fayz F., Eslami A. Determination of occlusal vertical dimension: a literature review. J Prosthet Dent. 1988. 59:321–3.
Article9.Willis FM. Features of the face involved in full denture prosthesis. Dent Cosmos. 1935. 77:851–4.10.Silverman MM. Determination of vertical dimension by phonetics. J Prosthetic Dent. 1956. 6:465–71.
Article11.Thompson JR. The rest position of the mandible and its significance to dental science. J Am Dent Assoc. 1946. 33:151–80.
Article12.Turner KA., Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984. 52:467–74.
Article13.de Jong MH., Wright PS., Meijer HJ., Tymstra N. Posterior mandibular residual ridge resorption in patients with overdentures supported by two or four endosseous implants in a 10-year prospective comparative study. Int J Oral Maxillofac Implants. 2010. 25:1168–74.14.Carlsson GE., Ingervall B., Kocak G. Effect of increasing vertical dimension on the masticatory system in subjects with natural teeth. J Prosthet Dent. 1979. 41:284–9.
Article15.Kim SO. Implant overdenture. Seoul: Myung Moon publishing;2007. p. 115–8. p. 344–50.16.Kleis WK., Ka¨mmerer PW., Hartmann S., Al-Nawas B., Wagner W. A comparison of three different attachment systems for mandibular two-implant overdentures: one-year report. Clin Implant Dent Relat Res. 2010. 12:209–18.
Article17.Sadig W. A comparative in vitro study on the retention and stability of implant-supported overdentures. Quintessence Int. 2009. 40:313–9.18.Hayakawa I., Hirano S. A method to remold worn acrylic resin posterior denture teeth and restore lost vertical dimension of occlusion. J Prosthet Dent. 1993. 69:234–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full mouth rehabilitation of the patient with severe tooth loss and tooth wear with vertical dimension gaining: A case report
- Full mouth rehabilitation of patient with decreased occlusal vertical dimension due to severely worn dentition and posterior bite collapse
- A case of full mouth rehabilitation with vertical dimension gaining in patient withseverely worn dentition and loss of vertical dimension due to loss of posterior support
- Full mouth rehabilitation accompanied by phonetic analysis of a patient with reduction of vertical dimension of occlusion, and inaccurate pronunciation due to numerous tooth loss: a case report
- Full mouth rehabilitation of the patient with severely worn dentition: a case report
