Korean J Urol.
2007 Jul;48(7):735-740. 10.4111/kju.2007.48.7.735.
The Characteristics of the Contralateral Inguinal Internal Ring and Hernia Sac by Transinguinal Laparoscopy in Boys with Unilateral Indirect Inguinal Hernia: Analysis of Risk Factors and Associated Features with Metachronous Development
- Affiliations
-
- 1Department of Urology, Eulji University College of Medicine, Daejeon, Korea. woosing@eulji.ac.kr
- KMID: 1990227
- DOI: http://doi.org/10.4111/kju.2007.48.7.735
Abstract
-
PURPOSE: We evaluated the contralateral patent processus vaginalis(CPPV) by transinguinal laparoscopy in boys with unilateral inguinal hernia, to determine its incidence and the association with various clinical parameters. We also investigated the factors responsible for the development of a metachronous inguinal hernia.
MATERIALS AND METHODS
One hundred sixty seven boys with unilateral inguinal hernia were analyzed. The morphology of the ring was classified into four patterns(type 1, 2a, 2b, and 3). We analyzed the morphology of the internal ring and the variables related to a CPPV by age, laterality and the size of the ipsilateral and/or bilateral hernia sac.
RESULTS
The incidence of a CPPV was 33.9%. The positive predictive value was 94.9%(56/59). There was no statistical difference in the incidence of a CPPV by laterality. The incidence of a CPPV was significantly higher in the group with a larger size(>or=1cm) compared to the smaller abnormalities(<1cm). The incidence of the type 3 pattern was higher than the type 2b pattern in the group with larger abnormalities. With increasing age, type 1 and 2a patterns increased in frequency, but type 2b decreased and the type 3 pattern was stable. The size of the contralateral hernia sac was significantly larger with the type 3 pattern than the type 2b.
CONCLUSIONS
The results of our study showed that the size of the hernia sac and patient age were related to the presence of a CPPV. A type 3 pattern was associated with a more primitive morphology, a wider hernia sac and no change in the incidence with advancing age. Therefore, the findings of this study suggest that a metachronous inguinal hernia develops more commonly in patients with a type 3 pattern internal ring.
Keyword
Figure
-

Fig. 1 The morphology of the internal inguinal ring (arrow: peritoneal veil).
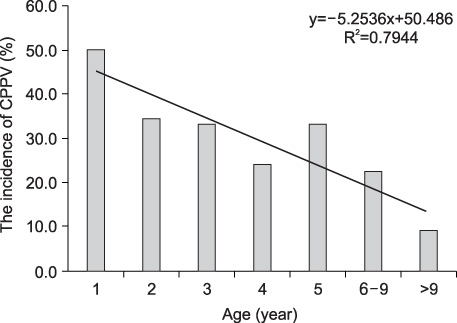
Fig. 2 The incidence of the contralateral patent processus vaginalis by age group. CPPV: contralateral patent processus vaginalis.
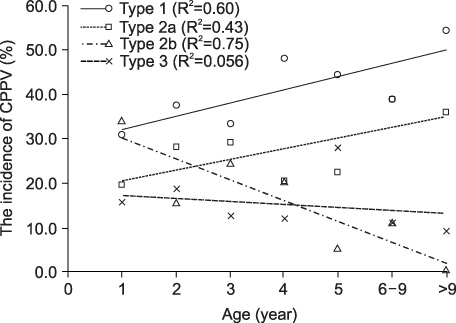
Fig. 3 The incidence and linear regression lines for the four types of contralateral inguinal rings by age. CPPV: contralateral patent processus vaginalis.
Reference
-
1. Bronsther B, Abrahams MW, Elbonim C. Inguinal hernia in children-a study of 1000 cases and a review of the literature. J Am Med Womens Assoc. 1972. 27:5222–5535.2. Matthyssens LE, Schwagten KJ, Vervloessem D, Verhelst AA. The contralateral inguinal hernia in children. J Pediatr Surg. 2005. 40:1058–1060.3. Miltenburg DM, Nuchtern JG, Jaksic T, Kozinetiz C, Brandt ML. Laparoscopic evaluation of the pediatric inguinal hernia-a meta-analysis. J Pediatr Surg. 1998. 33:874–879.4. Zitsman JL. Transinguinal diagnostic laparoscopy in pediatric inguinal hernia. J Laparoendosc Surg. 1996. 6:Suppl 1. S15–S20.5. Chin T, Liu C, Wei C. The morphology of the contralateral internal inguinal rings is age-dependent in children with unilateral inguinal hernia. J Pediatr Surg. 1995. 30:1663–1665.6. Fisher PC, Cartwright PC, Snow BW. Contralateral occurrence of hernia or hydrocele after unilateral hydrocele repair in children. J Urol. 2001. 165:Suppl. 193A. abstract 800.7. Ballantyne A, Jawaheer G, Munro FD. Contralateral groin exploration is not justified in infants with a unilateral inguinal hernia. Br J Surg. 2001. 88:720–723.8. Zona JZ. The incidence of positive contralateral inguinal exploration among preschool children-a retrospective and prospective study. J Pediatr Surg. 1996. 31:656–660.9. Miltenburg DM, Nuchtern JG, Jaksic T, Kozinetz CA, Brandt ML. Meta-analysis of the risk of metachronous hernia in infants and children. Am J Surg. 1997. 174:126–127.10. Kim DH, Ku JH, Lee NK. Epidemiologic study about inguinal hernia and hydrocele performed in young men in Daejeon city and Chung-nam area. Korean J Urol. 2002. 43:781–785.11. Rowe MI, Clatworthy HW. Incarcerated and strangulated hernia in children. A statistical study of high-risk factors. Arch Surg. 1970. 101:136–139.12. Ha YW, Yoon YR, Sul CK. Laparoscopy through the open ipsilateral sac to evaluate contralateral patent processus vaginalis in children with clinical unilateral inguinal hernia. Korean J Urol. 2001. 42:934–937.13. McGregor DB, Halverson K, McVay CB. The unilateral pediatric inguinal hernia: should the contralateral side be explored? J Pediatr Surg. 1980. 15:313–317.14. Nixon RG, Pope JC 4th, Adams MC, Holcomb GW 3rd, Brock JW 3rd. Laparoscopic variability of the internal inguinal ring: review of anatomical variation in children with and without a patent processus vaginalis. J Urol. 2002. 167:1818–1820.15. Moss RL, Hatch EI Jr. Inguinal hernia repair in early infancy. Am J Surg. 1991. 161:596–599.16. Manoharan S, Samarakkody U, Kulkarni M, Blakelock R, Brown S. Evidence-based change of practice in the management of unilateral inguinal hernia. J Pediatr Surg. 2005. 40:1163–1166.17. Ikeda H, Suzuki N, Takahashi A. Risk of contralateral manifestation in children with unilateral inguinal hernia: should hernia in children be treated contralaterally? J Pediatr Surg. 2000. 35:1746–1748.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Initial Experience with Percutaneous Internal Ring Suturing for Indirect Inguinal Hernia in Pediatric Patients
- Open Inguinal Hernia Repair with Transinguinal Laparoscopic Examination in Children: A 13 Years of Experience
- Laparoscopy Through the Open Ipsilateral Sac to Evaluate Contralateral Patent Processus Vaginalis in Children with Clinical Unilateral Inguinal Hernias
- Clinical Study of Contralateral Inguinal Hernia Development in Children with Unilateral Inguinal Hernia
- Contralateral Patent Processus Vaginalis in Unilateral Undescended Testis: Comparison between Preoperative Ultrasonographic and Transinguinal Laparoscopic Inspection
