Bilateral Femoral Neck Insufficiency Fractures after Use of a Long-term Anti-resorptive Drug Therapy for Osteoporosis: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul Sacred Heart General Hospital, Seoul, Korea. anectto@naver.com
- KMID: 1974390
- DOI: http://doi.org/10.5371/hp.2015.27.2.115
Abstract
- A 78-year-old woman developed an insufficiency fracture on her right femoral neck without trauma after four years of treatment with a bisphosphonate. Her fracture was fixed by two screws and her anti-osteoporotic drug was changed from an anti-resorptive to an anabolic agent. Seven months later, however, she sustained similar insufficiency fracture on the left femoral neck and was treated with the same method. She developed right inguinal pain again approximately eight months after her right side operation. The results of imaging tests revealed that her insufficiency fracture was converted to complete fracture, and that the fracture gap had widened as well. Her right hip was revised with hemiarthroplasty. A histological exam of the fracture site revealed evidence of decreased bone healing. Long-term administration of anti-resorptive drug prevents bone healing and remodeling and can result in atypical fractures of the femoral neck. Osteosynthesis was difficult to accomplish despite the application of proactive fixation. Therefore, more rigid fixation and careful postoperative treatment should be considered.
MeSH Terms
Figure
-
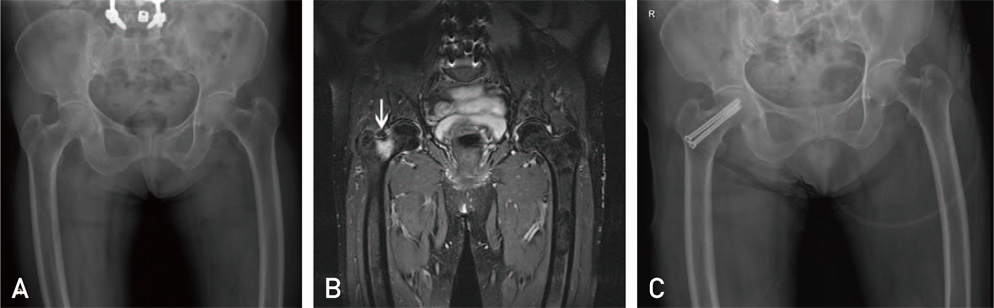
Fig. 1 (A) A plain radiograph shows no specific finding. (B) A magnetic resonance imaging T2 weighted image shows high signal bend (arrow) above the right femur neck. (C) A postoperative radiograph shows two well fixed cannulated hip screws.
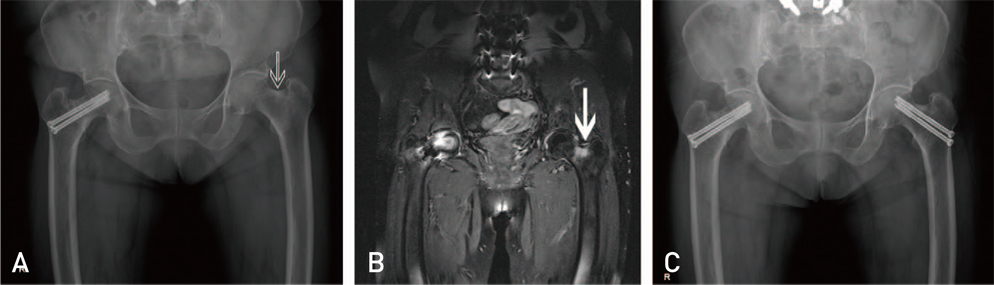
Fig. 2 (A) A plain radiograph shows sclerotic thickening (arrow) in the upper cortex of the left femoral neck. (B) A magnetic resonance imaging shows high signal lesion (arrow) above the left femur neck. (C) A postoperative radiograph shows two well-fixed cannulated screws.
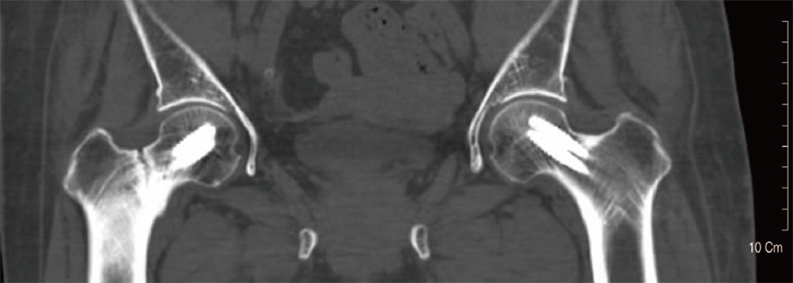
Fig. 3 A computed tomography scan shows a sclerotic fracture gap without union at the fatigue fracture site of the right femur neck. The two screws seem to be relatively well fixed.
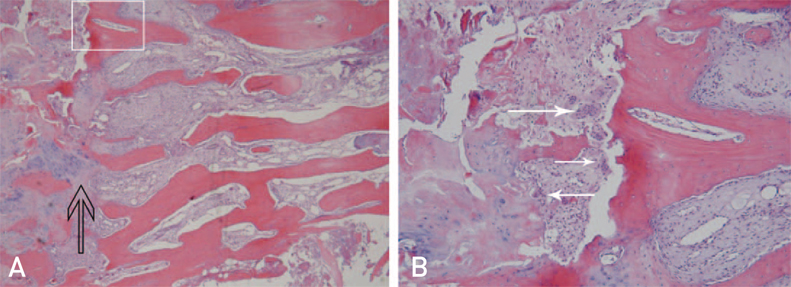
Fig. 4 (A) Histological findings of the fracture site (hematoxylin and eosin [H&E] stain, ×40). Multilayer thickened trabeculars of cancellous bone under the cortical bone can be seen, as well as cartilarge and fibrotic tissue in the portion of the fracture gap on the left (arrow). (B) The magnified (white square in A) histological findings (H&E stain, ×100) show some osteoclasts (arrows), chondrocytes, and a few osteoblasts on the fracture lesion. New bone formation can be seen, but at relatively low levels.
Cited by 1 articles
-
Acetabular Insufficiency Fracture Following Prolonged Alendronate Use and the Failure of Total Hip Arthroplasty in “Frozen” Bone: Two Cases Report
Sang-Joon Kwak, Yoon-Je Cho, Gwang-Young Jung, Joo-Hyun Lee, Young-Soo Chun, Kee-Hyung Rhyu
Hip Pelvis. 2017;29(4):286-290. doi: 10.5371/hp.2017.29.4.286.
Reference
-
1. Bone HG, Hosking D, Devogelaer JP, et al. Alendronate Phase III Osteoporosis Treatment Study Group. Ten years' experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med. 2004; 350:1189–1199.
Article2. Wasserman N, Yerramshetty J, Akkus O. Microcracks colocalize within highly mineralized regions of cortical bone tissue. Eur J Morphol. 2005; 42:43–51.
Article3. Kwek EB, Goh SK, Koh JS, Png MA, Howe TS. An emerging pattern of subtrochanteric stress fractures: a long-term complication of alendronate therapy? Injury. 2008; 39:224–231.
Article4. Soubrier M, Dubost JJ, Boisgard S, et al. Insufficiency fracture. A survey of 60 cases and review of the literature. Joint Bone Spine. 2003; 70:209–218.
Article5. Iwamoto J, Takeda T. Insufficiency fracture of the femoral neck during osteoporosis treatment: a case report. J Orthop Sci. 2002; 7:707–712.
Article6. Black DM, Cummings SR, Karpf DB. Fracture Intervention Trial Research Group. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet. 1996; 348:1535–1541.
Article7. Barrett J, Worth E, Bauss F, Epstein S. Ibandronate: a clinical pharmacological and pharmacokinetic update. J Clin Pharmacol. 2004; 44:951–965.
Article8. Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005; 90:1294–1301.
Article9. Park JG, Song KS, Jung HJ, Lee JS, Lee TJ, Kim KS. Bilateral femoral subtrochanteric insufficiency fractures after long-term bisphosphonate therapy. J Korean Orthop Assoc. 2010; 45:146–150.
Article10. Kim DH, Lee EC, Kang SK. Insufficiency fracture of ipsilateral femur neck in patient treated with long term bisphosphonate treatment - a case report -. J Bone Metab. 2012; 19:159–162.
Article11. Quinn SF, McCarthy JL. Prospective evaluation of patients with suspected hip fracture and indeterminate radiographs: use of T1-weighted MR images. Radiology. 1993; 187:469–471.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Insufficiency Fracture of Simultaneously Bilateral Femur Neck in Patient Treated with Long-Term Bisphosphonate Treatment - A Case Report -
- Sequential Bilateral Insufficiency Fractures of the Femur Neck in Patients Treated with Prolonged Bisphosphonate Therapy: A Case Report
- A Case Report of Long-Term Bisphosphonate Therapy and Atypical Stress Fracture of Bilateral Femur
- Insufficiency Fracture of Ipsilateral Femur Neck in Patient Treated with Long Term Bisphosphonate Treatment: A Case Report
- Insufficiency Fracture of the Femoral Neck after Intramedullary Nailing for the Treatment of Atypical Femoral Fracture - A Case Report -
