Tuberc Respir Dis.
2006 Dec;61(6):526-532. 10.4046/trd.2006.61.6.526.
Tuberculous Pleurisy: Clinical Characteristics of Primary and Reactivation Disease
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Dankook University, Chonan, Korea. jspark@dankook.ac.kr
- KMID: 1970237
- DOI: http://doi.org/10.4046/trd.2006.61.6.526
Abstract
-
BACKGROUND: Traditionally, tuberculous pleurisy has been known to largely develop as primary tuberculosis. However, as the incidence of tuberculosis decrease, recent studies have shown reactivation tuberculosis has become the main cause of tuberculous pleurisy.
METHODS
141 cases of tuberculous pleurisy, between January 2003 and February 2006, at the Dankook university hospital. were retrospectively studied. The patients were divided into primary and reactivation tuberculosis. based on the history and radiological characteristics, and the clinical, radiological characteristics at the time of diagnosis and residual pleural thickening after 6 month of chemotherapy were compared between the two groups.
RESULTS
1. Of the 141 tuberculous pleurisy cases, in 135 it was possible to differentiate between primary and reactivation tuberculosis. 2. Of the 135 tuberculous pleurisy cases, 38 (28%) showed a primary tuberculosis pattern, and 98 (72%) showed a reactivation tuberculosis pattern. 3. There were no significant differences between primary and reactivation tuberculosis in relation to age, sex, duration of symptom, amount of pleural effusion, pleural fluid WBC, lymphocyte count, and level of protein, LDH and ADA at the time of diagnosis. 4. 124 patients were followed for 6 months after diagnosis of tuberculous pleurisy, and there was no significant difference in the residual pleural thickening between primary and reactivation tuberculosis.
CONCLUSION
In South Korea, a reactivation disease is currently a more common cause of tuberculous pleurisy than a primary disease. There was no difference in the clinical characteristics between primary and reactivation tuberculosis.
Keyword
MeSH Terms
Figure
-
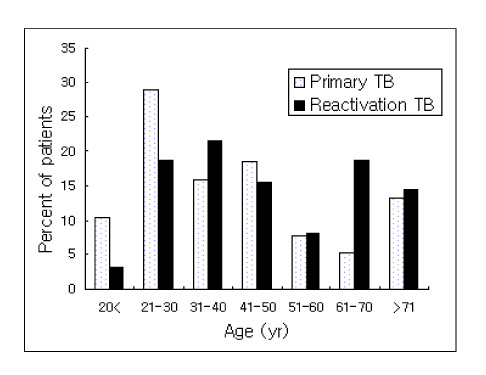
Figure 1 Percentage of patients according to age in both primary and reactivation tuberculosis.

Figure 2 Percentage of patients according to residual pleural thickening in both primary and reactivation tuberculosis. Residual pleural thickness was measured in the lower lateral hemithorax of a posteroanterior chest radiograph at the level of an imaginary line intersecting the diaphragm dome.
Reference
-
1. Mehta J, Dutt A, Harvill L, Mathews KM. Epidemiology of extrapulmonary tuberculosis. Chest. 1991. 99:1134–1138.2. Kim HJ, Lee KB, In KH, Kang KH, Yoo SH. A clinical study of exudative pleural effusion in the elderly. Tuberc Respir Dis. 1990. 37:300–305.3. Berger HW, Mejia E. Tuberculous pleurisy. Chest. 1973. 63:88–92.4. Abrams WB, Small MJ. Current concepts of tuberculous pleurisy with effusion as derived from pleural biopsy studies. Dis Chest. 1960. 38:60–65.5. Moudgil H, Sridhar G, Leitch A. Reactivation disease: the commonest form of tuberculous pleural effusion in Edinburgh, 1980-1991. Resp Med. 1994. 88:301–304.6. Valdes L, Alvarez D, San Jose E, Penela P, Valle JM, Carcia-Pazos JM, et al. Tuberculous pleurisy: a study of 154 patients. Arch Intern Med. 1998. 158:2017–2021.7. Ibrahim WH, Ghadban W, Khinji A, Yasin R, Soub H, Al-Khal AL, et al. Does pleural tuberculosis disease pattern differ among developed and developing countries. Resp Med. 2005. 99:1038–1045.8. Antoniskis D, Amin K, Barnes PF. Pleuritis as manifestation of reactivation tuberculosis. Am J Med. 1990. 89:447–450.9. Korea Center for Disease Control and Prevention. Korean Institute of Tuberculosis. Korean National Tuberculosis Association. 2005 annual report on the notified tuberculosis patients in Korea. 2006. Adopted from: www.Tbnet.nih.go.kr.10. Kim HJ, Lee HJ, Kwon SY, Yoon HI, Chung HS, Lee CT, et al. The prevalence of pulmonary parenchymal tuberculosis in patients with tuberculous pleuritis. Chest. 2006. 129:1253–1258.11. Flynn JL, Chan J. Immunology of tuberculosis. Annu Rev Immunol. 2001. 19:93–129.12. Arriero JM, Romero S, Hernandez L, Candela A, Martin C, Gil J, et al. Tuberculous pleurisy with or without radiographic evidence of pulmonary disease: is there any difference? Int J Tuberc Lung Dis. 1998. 2:513–517.13. de Pablo A, Villena V, Echave-Sustaeta J, Encuentra AL. Are pleural fluid parameters related to the development of residual pleural thickening in tuberculosis? Chest. 1997. 112:1293–1297.14. Candela A, Andujar J, Hernandez L, Martin C, Barroso E, Arriero JM, et al. Functional sequelae of tuberculous pleurisy in patients correctly treated. Chest. 2003. 123:1996–2000.15. Centers for Disease Control and Prevention(CDC). Trends in tuberculosis: United States, 2005. MMWR Morb Mortal Wkly Rep. 2006. 55:305–308.16. Aktogu S, Yorgancioglu A, Cirak K, Kose T, Dereli SM. Clinical spectrum of pulmonary and pleural tuberculosis, a report of 5480 cases. Eur Respir J. 1996. 9:2031–2035.17. Mihmanli A, Ozseker F, Baran A, Kucuker F, Atik S, Akkaya E. Evaluation of 105 cases with tuberculous pleurisy. Tuberk Toraks. 2004. 52:137–144.18. Small PM, Hopewell PC, Singh SP, Paz A, Parsonnet J, Ruston DC, et al. The epidemiology of tuberculosis in San Francisco: apopulation-based study using conventional and molecular methods. N Engl J Med. 1994. 330:1703–1709.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tuberculous Pleurisy: An Update
- A Study on pH and PCO2, in Tuberculous Pleurisy with Effusion
- A Case of Tuberculous Peritonitis Developed during Chemotherapy for Tuberculous Pleurisy as Paradoxical Response
- Diagnostic Efficacy of Adenosine Deaminase Isoenzyme in Tuberculous Pleurisy
- Soluble Interleukin-2 Receptor(sIL-2R) Levels in Patients Tuberculous Pleurisy VS Nontuberculous Pleurisy
