A Case of Tuberculous Peritonitis Developed during Chemotherapy for Tuberculous Pleurisy as Paradoxical Response
- Affiliations
-
- 1Department of Internal Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea. osbbang@paik.ac.kr
- KMID: 1792804
- DOI: http://doi.org/10.4166/kjg.2011.57.6.379
Abstract
- After the start of anti-tuberculous treatment, paradoxical worsening of tuberculous lesions has been described. However, abdominal tuberculosis as paradoxical response is relatively rare. This report describes the 26-year-old female who suffered from peritoneal tuberculosis while treating tuberculous pleurisy with anti-tuberculous medications. It was considered as paradoxical response, rather than treatment failure or else. She was successfully managed with continuing initial anti-tuberculous medications. When a patient on anti-tuberculous medications is presented with abdominal symptoms, the possibility of paradoxical response should be considered to avoid unnecessary tests and treatments, which may result in more suffering of the patient. Herein, we report a case of peritoneal tuberculosis as paradoxical response while treating tuberculous pleurisy.
Keyword
Figure
-
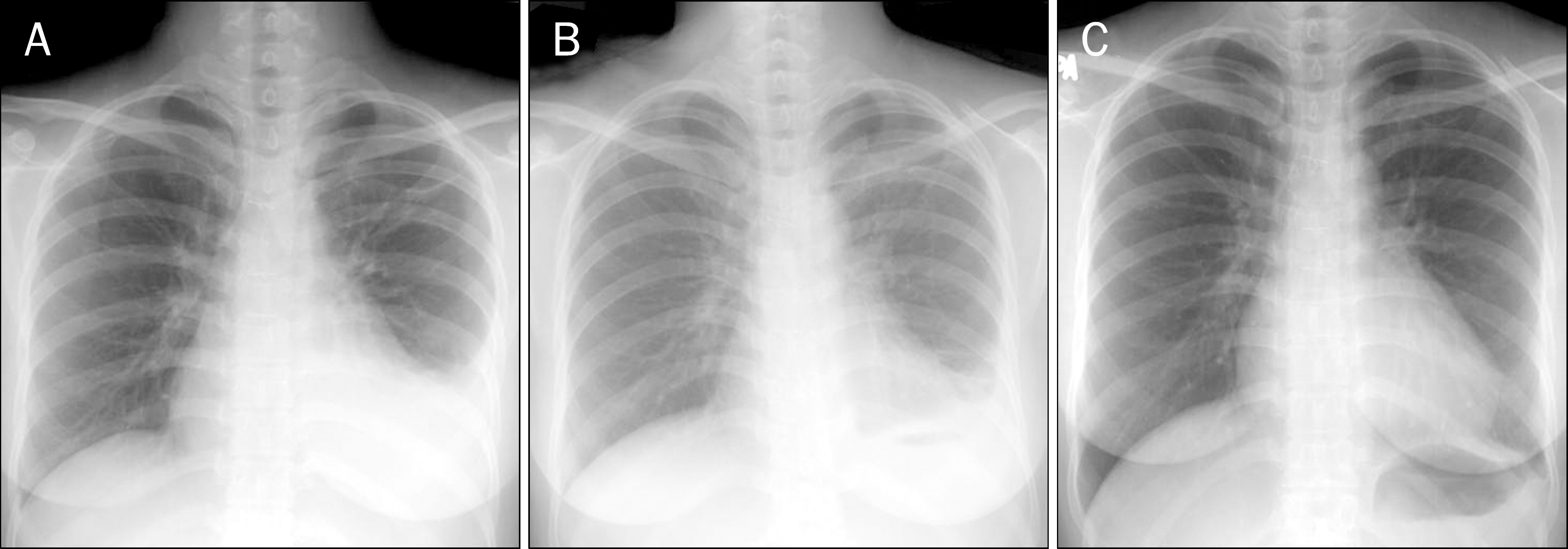
Fig. 1. Chest X-ray. (A) The initial chest X-ray showed left sided pleural effusion. (B) On admission, 10 weeks later, left sided pleural effusion was decreased. (C) Left sided pleural effusion was almost resolved 9 months after the start of antituberculous treatment.
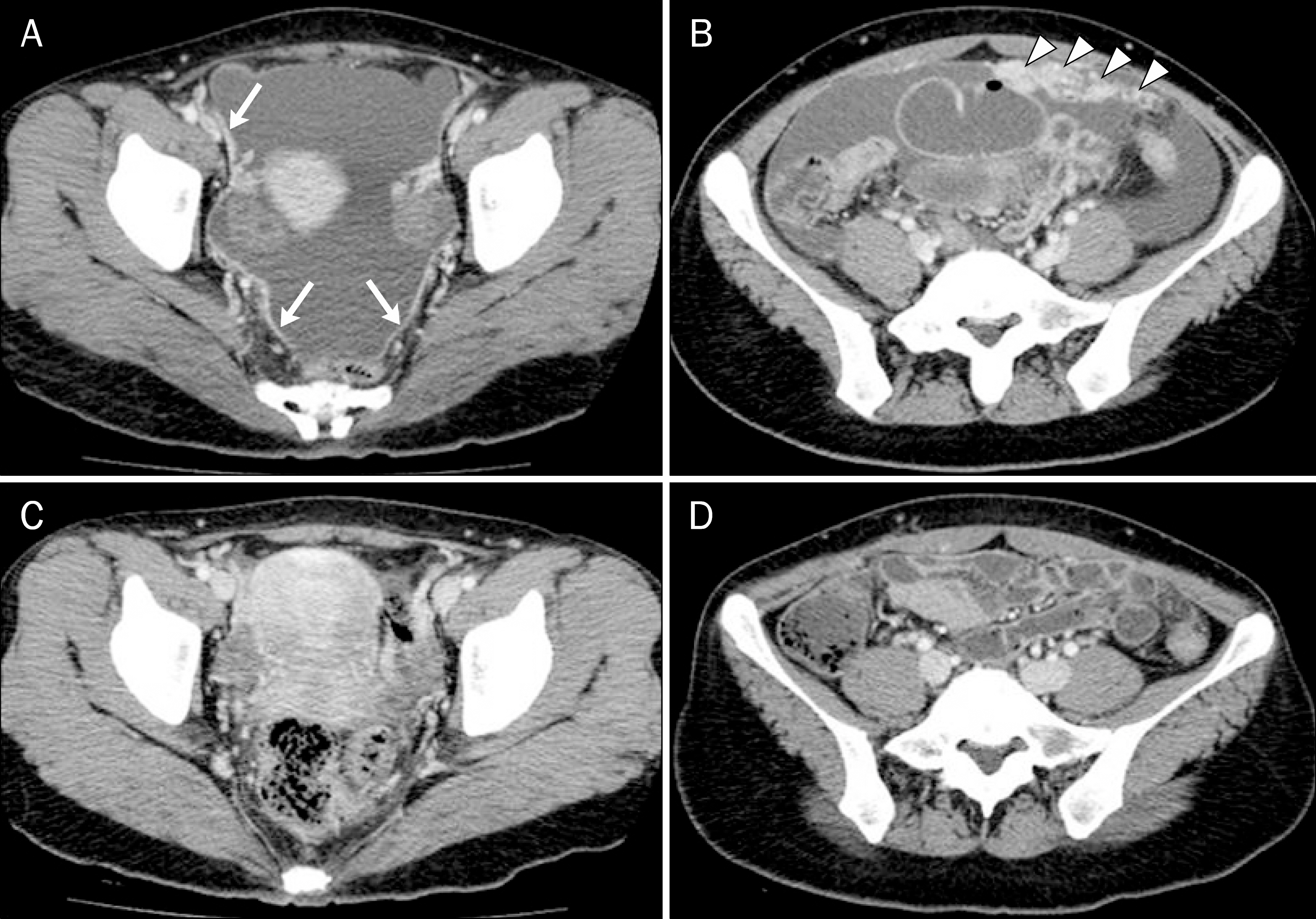
Fig. 2. Abdominal CT. Ascites and smooth uniform thickening with pronounced enhancement (arrows) and smudged pattern of the peritoneum (arrow heads), known as radiologically characteristic findings of tuberculous peritonitis, were shown (A, B). Ascites and the extent of smudged pattern of peritoneum disappeared 6 months after the start of antituberculous treatment (C, D).
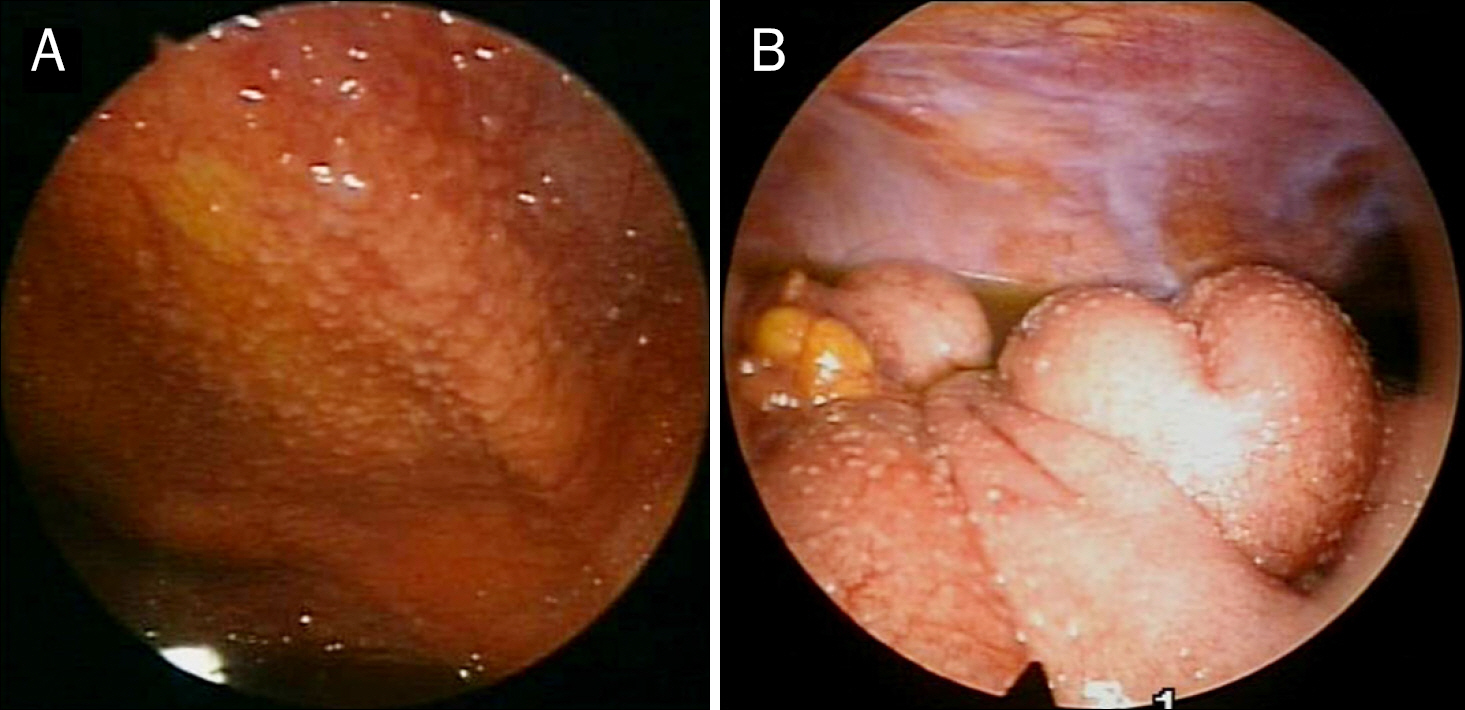
Fig. 3. Gross findings through the laparoscope. Diffuse whitish nodules with ascites were noted on the peritoneum and the intestines (A, B).
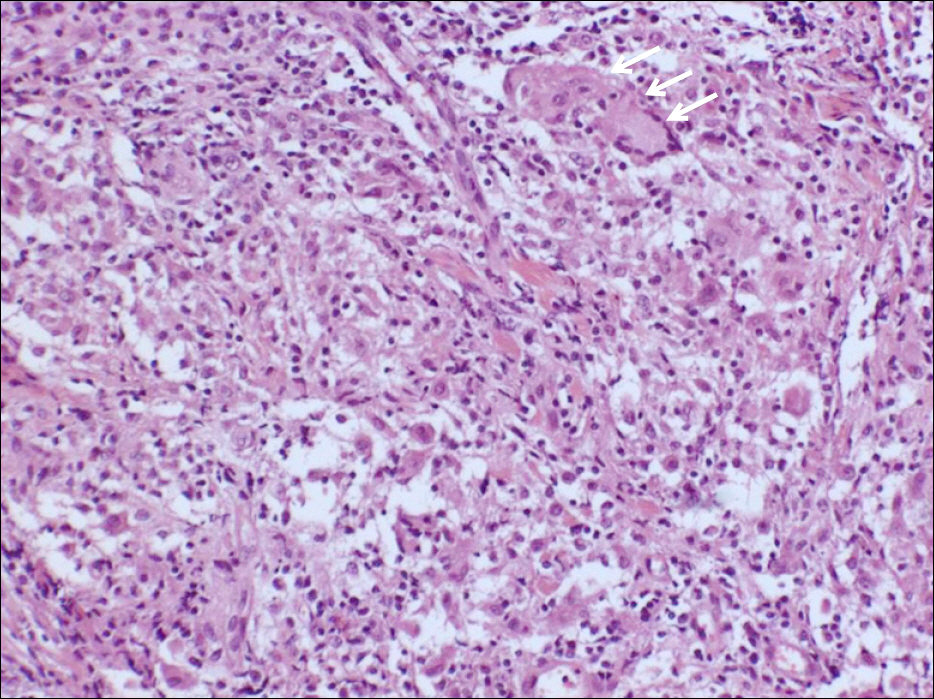
Fig. 4. Microscopic findings of peritoneum. Multinucleated giant cell (arrows) and chronic granulomas with epithelioid cells, consistent with tuberculous peritonitis, were noted (H&E, ×100).
Cited by 2 articles
-
A Case of Tuberculous Liver Abscess Developed during Chemotherapy for Tuberculous Peritonitis as Paradoxical Response
Tae Kyung Kim, Cheol Woong Choi, Jong Kun Ha, Hyung Ha Jang, Su Bum Park, Hyung Wook Kim, Dae Hwan Kang
Korean J Gastroenterol. 2013;62(1):64-68. doi: 10.4166/kjg.2013.62.1.64.A Case of Paradoxical Reaction Development during Antituberculosis Therapy
Young Bum Cho, Min Su Chu, Han Seung Ryu, Suck Chei Choi, Geom Seog Seo
Korean J Gastroenterol. 2015;65(5):306-311. doi: 10.4166/kjg.2015.65.5.306.
Reference
-
References
1. Demir K, Okten A, Kaymakoglu S, et al. Tuberculous peritonitis–reports of 26 cases, detailing diagnostic and therapeutic problems. Eur J Gastroenterol Hepatol. 2001; 13:581–585.2. Cheng VC, Ho PL, Lee RA, et al. Clinical spectrum of paradoxical deterioration during antituberculosis therapy in non-HIV-in-fected patients. Eur J Clin Microbiol Infect Dis. 2002; 21:803–809.
Article3. Blumberg HM, Burman WJ, Chaisson RE, et al. American thoracic society/centers for disease control and prevention/infectious diseases society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003; 167:603–662.4. Al-Majed SA. Study of paradoxical response to chemotherapy in tuberculous pleural effusion. Respir Med. 1996; 90:211–214.
Article5. Ahn TH, Park MB, Lee KJ, et al. A case report of tuberculous brain abscess and tuberculous peritonitis developing due to paradoxical reactions. Tuberc Respir Dis. 2009; 66:457–462.
Article6. Cheng VC, Yam WC, Woo PC, et al. Risk factors for development of paradoxical response during antituberculosis therapy in HIV-negative patients. Eur J Clin Microbiol Infect Dis. 2003; 22:597–602.
Article7. Meintjes G, Rangaka MX, Maartens G, et al. Novel relationship between tuberculosis immune reconstitution inflammatory syndrome and antitubercular drug resistance. Clin Infect Dis. 2009; 48:667–676.
Article8. Song EJ, Baek DH, Jung JY, et al. Paradoxical response developed during the antituberculous treatment in tuberculous pleurisy. Tuberc Respir Dis. 2008; 64:427–432.
Article9. Kim JY, Kwon JH, Kim MJ, et al. Paradoxical response during antituberculous treatment for abdominal tuberculosis. J Korean Radiol Soc. 2006; 55:599–605.
Article10. Kasahara K, Fukuoka A, Murakawa K, et al. Tuberculous peritonitis developing during chemotherapy for pulmonary and intestinal tuberculosis: a case report. Respirology. 2005; 10:257–260.
Article11. Ha CY, Kim JY, Kim GC, et al. An intraperitoneal tuberculous abscess: Computed tomography (CT) findings and clinical course. Korean J Med. 2008; 74:243–249.12. Lee JS, Kim KA, Lee WJ, et al. Diagnostic value of ascitic fluid adenosine deaminase activity for diagnosis of tuberculous peritonitis. Korean J Gastroenterol. 2003; 41:126–132.13. Kim KS, Pyon YJ, Seong KC, et al. A case with chylous ascites fol-lowed by tuberculous peritonitis. Korean J Gastroenterol. 1997; 29:847–852.14. Jung MK, Lee HJ, Kim MJ, et al. Paradoxical response to chemotherapy in tuberculous pleural effusion. Pediatr Allergy Respir Dis. 2009; 19:71–77.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The CT findings and clinical course of intraperitoneal tuberculous abscess
- A Case of Tuberculous Liver Abscess Developed during Chemotherapy for Tuberculous Peritonitis as Paradoxical Response
- A Case Report of Tuberculous Brain Abscess and Tuberculous Peritonitis Developing Due to Paradoxical Reactions
- Paradoxical Response Developed during the Antituberculous Treatment in Tuberculous Pleurisy
- A case of newly developed pulmonary lesion during the antitubercular agents in tuberculous pleurisy : A paradoxical response
