Effects of the Balance Control Training in Chronic Hemiplegic Stroke Patients
- Affiliations
-
- 1Department of Rehabilitation Medicine, Dae-gu Fatima Hospital, 1Department of Rehabilitation Medicine, Kyung Pook National University College of Medicine, Korea. naftacho@hanmail.net
- KMID: 1965896
- DOI: http://doi.org/10.12786/bn.2012.5.1.32
Abstract
OBJECTIVE
To investigate the training effects on balance and gait ability using balance control trainer combined with partial weight-bearing system in chronic hemiplegic stroke patients. METHOD: A prospective crossover clinical trial was designed. The subjects consisted of 16 chronic hemiplegic stroke patients. All patients had a stroke more than six months. In addition to conventional physical therapy (PT), 8 patients in group A were trained with the balance control trainer for 30 min/day, 5 day/week, for first 2 weeks and then received only conventional physical therapy for 2 weeks. The other 8 patients in group B received only conventional PT for first 2 weeks and then were trained with the balance control trainer for 30 min/day, 5 day/week, for next 2 weeks, with additional conventional PT. We evaluated with clinical tests including functional ambulation categories (FAC), Berg balance scale (BBS), 6 min walking distance (6mWT), timed up and go (TUG), Korean-modified barthel Index (K-MBI) and muscle strengthening of knee extensor (MMTknee) before training, 2 weeks and 4 weeks after training in those patients.
RESULTS
After training, subjects in experimental period (2weeks period of conventional PT+Balance control trainer in group A&B) showed more improvement than those in control period (2 weeks period of only conventional PT in group A&B) in FAC, BBS, 6mWT, TUG, K-MBI (p<0.05).
CONCLUSION
We think the balance control trainer combined with the partial weight-bearing system can be a useful tool for improving balance and gait ability in chronic hemiplegic stroke patients.
Keyword
Figure
-
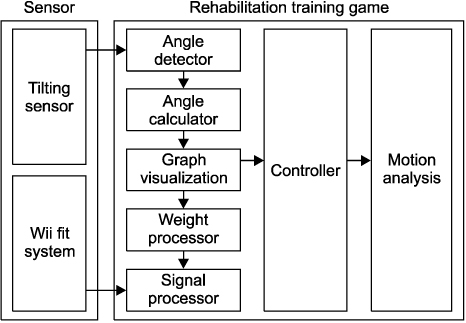
Fig. 1 Configuration of balance control trainer of lower extremity.
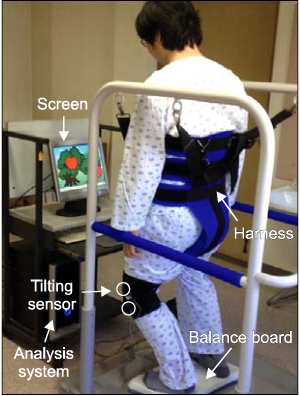
Fig. 2 The balance control trainer of lower extremity consists of the Wii fit balance board which detects the degree of weight shifting to right or left side, tilting sensor which detects the degree of affected knee flexion, and the computerized system which enables to perform the apple harvesting game using these data.
Fig. 3 The wii-fit balance board system has bluetooth and contains multiple pressure sensors that are used to measure the user's COP (center of pressure)-the location of the intersection between an imaginary line drawn vertically through the center of mass and the surface of the balance boardand weight. The sensors on the board can accurately measure up to 150 kg (330 pounds).
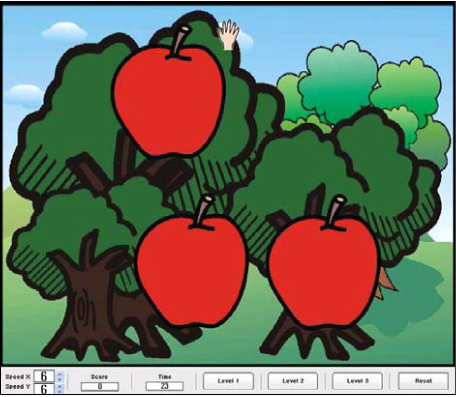
Fig. 4 This figure shows the apple harvesting game. According to weight shift to either side, the hand moves to right or left side, and according to the degree of knee flexion, the hand moves up or down side. When the hand touch apples on screen, apples disappear. When all apples have disappeared, apples re-appear on the screen randomly, and new game started.
Reference
-
1. Brandstater ME, Bruin H, Gowland C, Clark BM. Hemiplegic gait: analysis of temporal variables. Arch Phys Med Rehabil. 1983. 64:583–587.2. Moseley AM, Stark A, Cameron ID, Pollock A. Treadmill training and body weight support for walking after stroke. Cochrane Database Syst Rev. 2005. (4):CD002840.3. Lorish TR, Sandin KJ, Roth EJ, Noll SF. Stroke rehabilitation: 3. rehabilitation evaluation and management. Arch Phys Med Rehabil. 1994. 75:S47–S51.4. Patton J, Brown DA, Peshkin M, Santos-Munné JJ, Makhlin A, Lewis E, Colgate EJ, Schwandt D. Design and development of a robotic overgroud gait and balance therapy device. Top Stroke Rehabil. 2008. 15:131–139.5. Mayr A, Kofler M, Quirbach E, Matzak H, Frohlich K, Saltuari L. Prospective, blinded, randomized crossover study of gait rehabilitation in stroke patients using the lokomat gait orthosis. Neurorehabil Neural Repair. 2007. 21:307–314.6. Husemann B, Muller F, Krewer C, Heller S, Koeniq E. Effects of locomotion training with assistance of a robot-driven gait orthosis in hemiparetic patients after stroke: a randomized controlled pilot study. Stroke. 2007. 38:349–354.7. Lim KB, Na YM, Lee HJ, Hwang HO. Effect of balance board training with tactile stimulation on affected leg in hemiplegic patient. J Korean Acad Rehabil Med. 2002. 26:652–657.8. Nichols DS. Balance retraining after stroke using force platform biofeedback. Phys Ther. 1997. 77:553–558.9. Liston RAL, Brouwer B. Reliability and validity of measures obtained from stroke patients using the Balance Master. Arch Phys Med Rehabil. 1996. 77:425–430.10. Shumway-Cook A, Woollacott MH. Motor control: translating research into clinical practice. 2007. 3rd ed. Philadelphia: Lippincott Williams & Wilkins;3–83.11. Barclay-Goddard R, Stevenson T, Poluha W, Moffatt ME, Taback SP. Force platform feedback for standing balance training after stroke. Cochrane Database Syst Rev. 2004. (4):CD004129.12. Richards CL, Malouin F, Wood-Dauphinee S, Williams JI, Bouchard JP, Brunet D. Task-specific physical therapy for optimization of gait recovery in acute stroke patients. Arch Phys Med Rehabil. 1993. 74:612–620.13. Winstein CJ. Knowledge of results and motor-learning-implications for physical therapy. Phys Ther. 1991. 71:140–149.14. Dickstein R, Nissan M, Pillar T, Scheer D. Foot-ground pressure pattern of standing hemiplegic patients-major characteristics and patterns of involvement. Phys Ther. 1984. 64:19–23.15. De Haart M, Geurts AC, Dault MC, Nienhuis B, Duysens J. Restoration of weight-shifting capacity in patients with postacute stroke: a rehabilitation cohort study. Arch Phys Med Rehabil. 2005. 86:755–762.16. Winstein CJ, Gardner ER, McNeal DR, Barto PS, Nicholison DE. Standing balance training: effect on balance and locomotion in hemiparetic adults. Arch Phys Med Rehabil. 1989. 70:755–762.17. Nichols DS. Balance retraining after stroke using force platform biofeedback. Phys Ther. 1997. 77:553–558.18. Liston RAL, Brouwer B. Reliability and validity of measures obtained from stroke patients using the Balance Master. Arch Phys Med Rehabil. 1996. 77:425–430.19. Winstein CJ, Gardner ER, McNeal DR, Barto PS, Nicholison DE. Standing balance training: effect on balance and locomotion in hemiparetic adults. Arch Phys Med Rehabil. 1989. 70:755–762.20. Nichols DS. Balance retraining after stroke using force platform biofeedback. Phys Ther. 1997. 77:553–558.21. Betker AL, Szturm T, Moussavi ZK, Nett C. Video game-based exercises for balance rehabilitation: a single-subject design. Arch Phys Med Rehabil. 2006. 87:1141–1149.22. Geiger RA, Allen JB, O'Keefe J, Hicks RR. Balance and mobility following stroke: effects of physical therapy interventions with and without biofeedback/forceplate training. Phys Ther. 2001. 81:995–1006.23. Walker C, Brouwer Bj, Culham EG. Use of visual feedback in retraining balance following acute stroke. Phys Ther. 2000. 80:886–895.24. Barclay-Goddard R, Stevenson T, Poluha W, Moffatt ME, Taback SP. Force platform feedback for standing balance training after stroke. Cochrane Database Syst Rev. 2004. (4):CD004129.25. Mirbagheri MM, Tsao C, Settle K, Lilaonitkul T, Rymer WZ. Time course of changes in neuromuscular properties following stroke. Conf Proc IEEE Eng Med Biol Soc. 2008. 2008:5097–5100.26. Kriz J, Lalancette-Hébert M. Inflammation, plasticity and real-time imaging after cerebral ischemia. Acta Neuropathol. 2009. 117:497–509.27. Takatsuru Y, Fukumoto D, Yoshitomo M, Nemoto T, Tsukada H, Nabekura J. Neuronal circuit remodeling in the contralateral cortical hemisphere during functional recovery from cerebral infarction. J Neurosci. 2009. 29:10081–10086.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effects of Balance Training Using Balance System in the Hemiplegic Patients
- Effects of Treadmill Gait Training According to Different Inclination on Postural Balance in Patients with Chronic Stroke
- The Effects of Additional Balance Training in Subacute Hemiplegic Stroke Patients
- Effects of 3-Dimensional Lumbar Stabilization Training for Balance in Chronic Hemiplegic Stroke Patients: A Randomized Controlled Trial
- Effect of Balance Board Training with Tactile Stimulation on Affected Leg in Hemiplegic Patient
