J Korean Foot Ankle Soc.
2014 Mar;18(1):29-35. 10.14193/jkfas.2014.18.1.29.
Results of Syndesmotic Screw Fixation versus Posterior Malleolus Fixation in Syndesmotic Injury at Pronation External Rotation Stage IV Ankle Fracture with Posterior Malleolus Fracture: Postoperative One Year Follow-up
- Affiliations
-
- 1Department of Orthopedic Surgery, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. qortn97@naver.com
- KMID: 1958736
- DOI: http://doi.org/10.14193/jkfas.2014.18.1.29
Abstract
- PURPOSE
The purpose of this study is to compare the radiologic and clinical results of syndesmotic screw fixation and posterior malleolar fixation for syndesmotic injury in Lauge-Hansen classification pronation-external rotation (PER) stage IV ankle fractures with posterior malleolus fracture.
MATERIALS AND METHODS
We designed a retrospective study that included patients with Lauge-Hansen classification PER stage IV ankle fracture with posterior malleolus fracture. Of 723 patients who underwent ankle fracture surgery from March 2005 to November 2012, 29 were included in this study. In this study, syndesmotic injury was treated with syndesmotic screw fixation or posterior malleolus fixation. There were 15 cases of syndesmotic screw fixation and 14 cases of posterior malleolar fixation. We compared the radiologic and clinical results at one year postoperatively. Posterior malleolus fragment size on a pre-operative computed tomographic image, and tibiofibular overlap, medial clear space, articular step-off, Kellgren-Lawrence grade, and Takakura classification on a postoperative one year followup radiograph were used for comparison of the radiologic results. The clinical results were assessed using the American Orthopaedic Foot and Ankle Society score, visual analogue scale score, and patient subjective satisfaction score.
RESULTS
Posterior malleolar fragment size was 12.62%+/-3.01% of the joint space in the syndesmotic screw fixation group and 27.04%+/-4.34% in the posterior malleolar fixation group. A statistical difference was observed between the two groups. However, other results, including tibiofibular overlap, medial clear space, articular step-off, Kellgren-Lawrence grade, Takakura classification, and clinical scores showed no statistical difference.
CONCLUSION
In the Lauge-Hansen classification PER stage IV ankle fracture with posterior malleolus fracture, if the posterior malleolus fracture can be reduced anatomically and fixated rigidly, syndesmotic screw fixation, which can cause several complications, is usually not required for achievement of a satisfactory syndesmotic stability; this would be a recommendable option for treatment of syndesmotic injury.
MeSH Terms
Figure
-
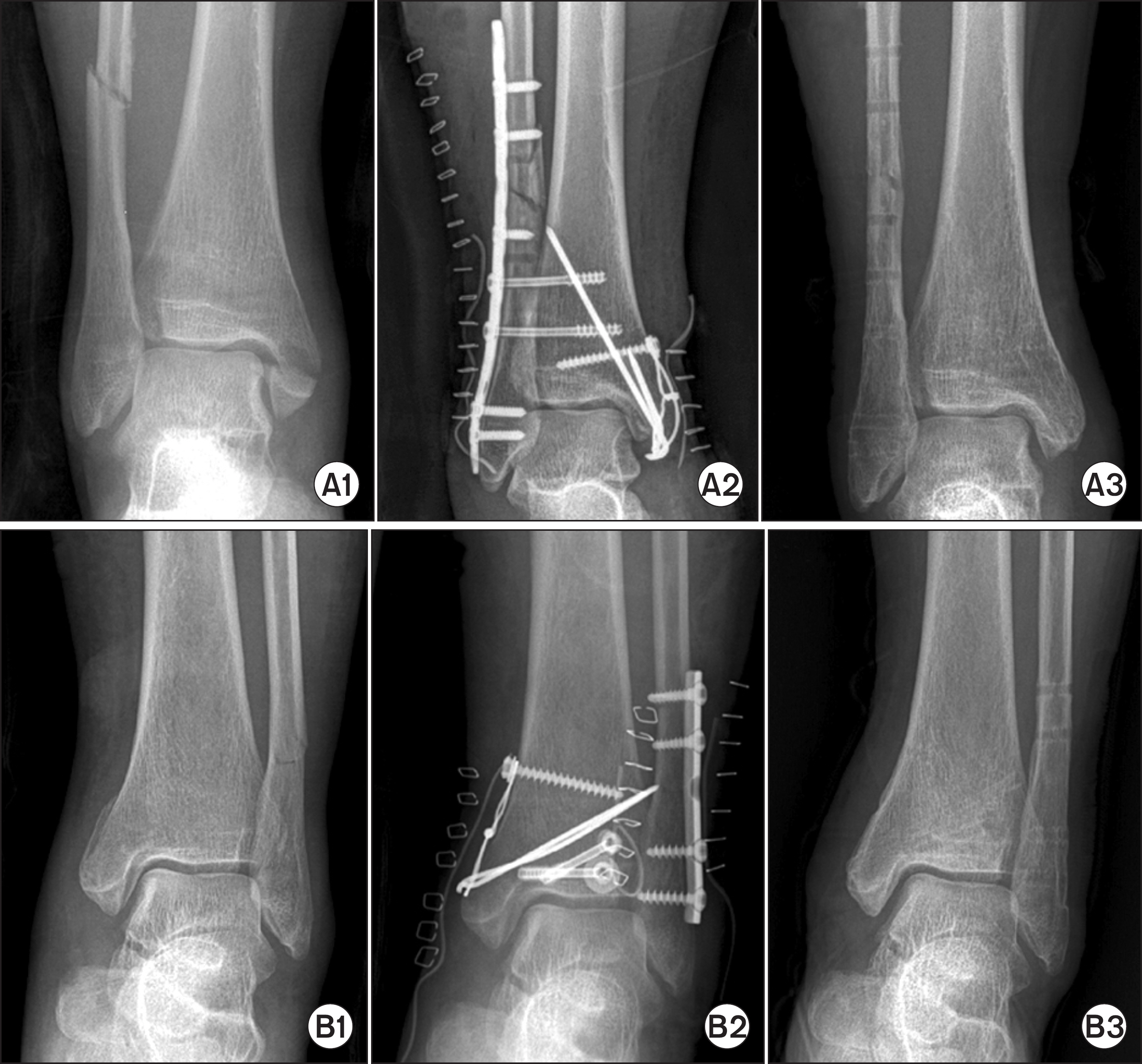
Figure 1. Radiologic examination of two group was reviewed. A1, B1: preoperative radiograph, A2, B2: immediate postoperative radiograph, A3, B3: radiograph at one year after operation.
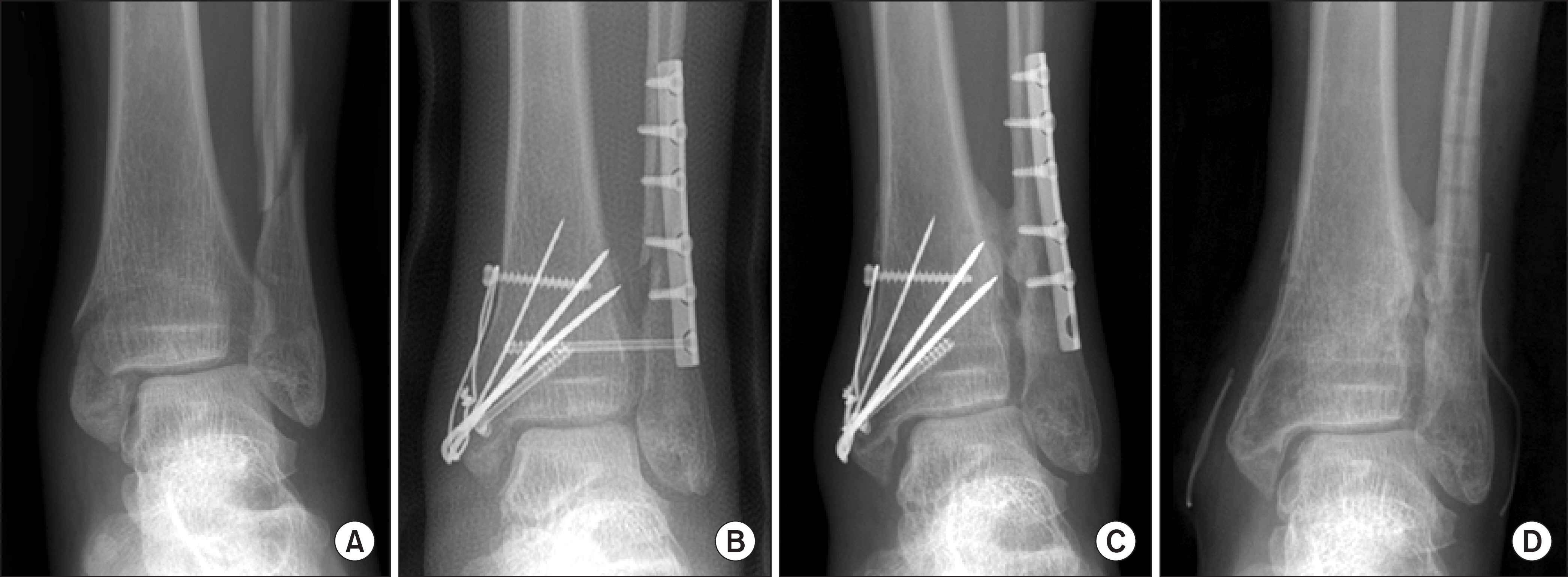
Figure 2. Distal tibiofibular synostosis after syndesmotic screw fixation was seen. (A) Preoperative radiograph of pronation-external rotation stage IV ankle fracture. (B) Immediate postoperative radiograph. (C) Radiograph at one year after operation. (D) Radiograph after implant removal.
Reference
-
References
1. Fritschy D. An unusual ankle injury in top skiers. Am J Sports Med. 1989; 17:282–5.
Article2. Hopkinson WJ, St Pierre P, Ryan JB, Wheeler JH. Syndesmosis sprains of the ankle. Foot Ankle. 1990; 10:325–30.
Article3. Rasmussen O. Stability of the ankle joint. Analysis of the function and traumatology of the ankle ligaments. Acta Orthop Scand Suppl. 1985; 211:1–75.4. Herscovici D Jr, Anglen JO, Archdeacon MT, Cannada LK, Scaduto JM. Avoiding complications in the treatment of pronation-external rotation ankle fractures, syndesmotic injuries, and talar neck fractures. Instr Course Lect. 2009; 58:37–45.5. Boden SD, Labropoulos PA, McCowin P, Lestini WF, Hurwitz SR. Mechanical considerations for the syndesmosis screw. A cadaver study. J Bone Joint Surg Am. 1989; 71:1548–55.
Article6. Farhan MJ, Smith TW. Fixation of diastasis of the inferior tibiofibular joint using the syndesmosis hook. Injury. 1985; 16:309–11.
Article7. Xenos JS, Hopkinson WJ, Mulligan ME, Olson EJ, Popovic NA. The tibiofibular syndesmosis. Evaluation of the ligamentous structures, methods of fixation, and radiographic assessment. J Bone Joint Surg Am. 1995; 77:847–56.
Article8. Yde J, Kristensen KD. Inferior tibiofibular diastasis treated by staple fixation. J Trauma. 1981; 21:483–5.9. Amendola A. Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle. 1992; 13:44–50.
Article10. Needleman RL, Skrade DA, Stiehl JB. Effect of the syndesmotic screw on ankle motion. Foot Ankle. 1989; 10:17–24.
Article11. Stiehl JB. Complex ankle fracture dislocations with syndesmotic diastasis. Orthop Rev. 1990; 19:499–507.12. Ogilvie-Harris DJ, Reed SC, Hedman TP. Disruption of the ankle syndesmosis: biomechanical study of the ligamentous restraints. Arthroscopy. 1994; 10:558–60.
Article13. Gardner MJ, Brodsky A, Briggs SM, Nielson JH, Lorich DG. Fixation of posterior malleolar fractures provides greater syndesmotic stability. Clin Orthop Relat Res. 2006; 447:165–71.
Article14. Gardner MJ, Demetrakopoulos D, Briggs SM, Helfet DL, Lorich DG. Malreduction of the tibiofibular syndesmosis in ankle fractures. Foot Ankle Int. 2006; 27:788–92.
Article15. Miller AN, Carroll EA, Parker RJ, Helfet DL, Lorich DG. Posterior malleolar stabilization of syndesmotic injuries is equivalent to screw fixation. Clin Orthop Relat Res. 2010; 468:1129–35.
Article16. Xu HL, Li X, Zhang DY, Fu ZG, Wang TB, Zhang PX, et al. A retrospective study of posterior malleolus fractures. Int Orthop. 2012; 36:1929–36.
Article17. Chissell HR, Jones J. The influence of a diastasis screw on the outcome of Weber type-C ankle fractures. J Bone Joint Surg Br. 1995; 77:435–8.
Article18. Rasmussen O, Tovborg-Jensen I, Boe S. Distal tibiofibular ligaments. Analysis of function. Acta Orthop Scand. 1982; 53:681–6.19. Bae SY, Sohn SE, Seong MK. The impacts of fixation tightness and duration on the remnant syndesmotic widening and clinical symptom after removal of screws. J Korean Foot Ankle Soc. 2013; 17:264–71.20. Harper MC. Ankle fracture classification systems: a case for integration of the Lauge-Hansen and AO-Danis-Weber schemes. Foot Ankle. 1992; 13:404–7.
Article21. Solari J, Benjamin J, Wilson J, Lee R, Pitt M. Ankle mortise stability in Weber C fractures: indications for syndesmotic fixation. J Orthop Trauma. 1991; 5:190–5.22. Peter RE, Harrington RM, Henley MB, Tencer AF. Biomechanical effects of internal fixation of the distal tibiofibular syndesmotic joint: comparison of two fixation techniques. J Orthop Trauma. 1994; 8:215–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prediction of Syndesmotic Instability according to the Lateral Malleolus Fracture Pattern in Supination-External Rotation Type Ankle Fractures: Short Oblique versus Long Oblique Fracture
- What is the Significance of the Posterior Malleolus in Ankle Fractures?
- Comparative analysis for syndesmotic Fixation vs Non-syndesmotic Fixation of distal Tibiofibular Diastasis
- The Effect of Syndesmotic Screw of Ankle Fracture with Distal Tibiofibular Diastasis
- Comparative Analysis of Trans-syndesmotic Versus Non-syndesmotic Screw Fixation in Surgical Treatment of Ankle Fracture with Diastasis
