J Korean Med Assoc.
2006 Apr;49(4):313-320. 10.5124/jkma.2006.49.4.313.
Clinical History and Diagnosis of Chronic Obstructive Pulmonary Disease
- Affiliations
-
- 1Division of Pulmonary and Allergology/Department of Internal Medicine, Yeungnam University College of Medicine and Hospital, Korea. ghlee@med.yu.ac.kr
- KMID: 1958285
- DOI: http://doi.org/10.5124/jkma.2006.49.4.313
Abstract
- Patients with COPD typically present when they are older than 50 years of age, and about 80% of them are male. Clinically the patients with COPD present with cough, sputum, and dyspnea that are gradually progressive over years. Other symptoms are wheezing, hemoptysis, and chest tightness. In many patients with COPD, physical examination reveals no significant findings especially during quiet breathing. As the disease becomes more severe, patients demonstrate more apparent physical signs. The assessment of the lung function is essential to establish the diagnosis and to determine the severity of COPD. The spirometry is the most important test for diagnosing and staging COPD. Office spirometry is a feasible testing strategy to diagnose patients with the early stage of COPD and may be used to encourage smoking cessation. The Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) recommends to define the severity of COPD and a stepwise approach for the management of COPD.
Keyword
MeSH Terms
Figure
-

Figure 1 Pulmonary function test in patients with COPD

Figure 2 Chest X-ray of emphysema

Figure 3 Chest X-ray of chronic bronchitis
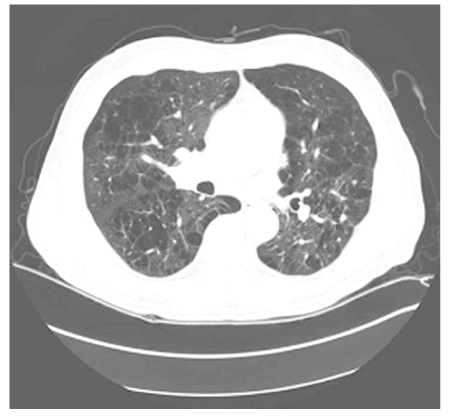
Figure 4 Chest C-T scan of emphysema
Reference
-
1. Shapiro SD, Snider GL, Rennard SI. Murray JF, Nadal JA, editors. Chronic bronchitis and emphysema. Textbook of Respiratory Medicine. 2005. 4th ed. Philadelphia: WB Saunders;1115–1125.
Article4. Reilly J, Silverman EK, Shapiro SD. Braunwald E, Fauci AS, Kasper D, Hauser SL, Longo DL, Jameson JL, editors. Chronic Obstructive Pulmonary Disease. Harrison's Principles of Internal Medicine. 2005. 16th ed. New York: McGraw-Hil;1147–1150.5. Anthonisen N. Goldman L, Bennett JC, editors. Chronic Obstructive Pulmonary Disease. Cecil textbook of medicine. 2005. 22nd ed. Philadelphia: WB Saunders;509–515.6. American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1995. 152:S77–S121.7. Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004. 23:932–946.
Article8. Kanner RE, Connett JE, Williams DE, Buist AS. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: the Lung Health Study. Am J Med. 1999. 106:410–416.
Article9. Badgett RG, Tanaka DJ, Hunt DK, Jelley MJ, Feinberg LE, Petty TL, et al. Can moderate chronic obstructive pulmonary disease be diagnosed by historical and physical findings alone? Am J Med. 1993. 94:188–196.
Article10. Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Lung Disease. NHLBI/WHO workshop report. 2001. 04. Date updated: 1 July 2003. Bethesda: National Heart, Lung and Blood Institute;Updte of the Management Sections, GOLD website www.goldcopd.com.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical History and Diagnosis of Chronic Obstructive Pulmonary Disease (COPD)
- Cor Pulmonale with Particular Reference to Chronic Obstructive Pulmonary Disease and Pulmonary Tuberculosis
- Chronic Obstructive Pulmonary Disease: Respiratory Review of 2014
- Management of Chronic Obstructive Pulmonary Disease
- Pathophysiology of Chronic Obstructive Pulmonary Disease
