J Korean Neurosurg Soc.
2014 Aug;56(2):114-120. 10.3340/jkns.2014.56.2.114.
Cervical Cord Decompression Using Extended Anterior Cervical Foraminotomy Technique
- Affiliations
-
- 1Department of Neurosurgery, Konyang University Hospital, Daejon, Koera. endoneurocare@gmail.com
- 2Department of Neurosurgery, Teun Teun Hospital, Daejon, Korea.
- KMID: 1956513
- DOI: http://doi.org/10.3340/jkns.2014.56.2.114
Abstract
OBJECTIVE
At present, gold-standard technique of cervical cord decompression is surgical decompression and fusion. But, many complications related cervical fusion have been reported. We adopted an extended anterior cervical foraminotomy (EACF) technique to decompress the anterolateral portion of cervical cord and report clinical results and effectiveness of this procedure.
METHODS
Fifty-three patients were operated consecutively using EACF from 2008 to 2013. All of them were operated by a single surgeon via the unilateral approach. Twenty-two patients who exhibited radicular and/or myelopathic symptoms were enrolled in this study. All of them showed cervical cord compression in their preoperative magnetic resonance scan images.
RESULTS
In surgical outcomes, 14 patients (64%) were classified as excellent and six (27%), as good. The mean difference of cervical cord anterior-posterior diameter after surgery was 0.92 mm (p<0.01) and transverse area was 9.77 mm2 (p<0.01). The dynamic radiological study showed that the average post-operative translation (retrolisthesis) was 0.36 mm and the disc height loss at the operated level was 0.81 mm. The change in the Cobb angle decreased to 3.46, and showed slight kyphosis. The average vertebral body resection rate was 11.47%. No procedure-related complications occurred. Only one patient who had two-level decompression needed anterior fusion at one level as a secondary surgery due to postoperative instability.
CONCLUSIONS
Cervical cord decompression was successfully performed using EACF technique. This procedure will be an alternative surgical option for treating cord compressing lesions. Long-term follow-up and a further study in larger series will be needed.
Keyword
MeSH Terms
Figure
-
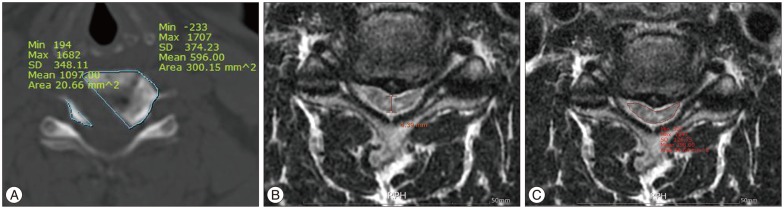
Fig. 1 Sketch diagram of measurement of vertebral body resection area (A), AP diameter (B), and transverse area (C) by TeraRecon Workstation.

Fig. 2 A and B : Axial, T2-weighted, MRI scans demonstrated C4-5, C5-6 disc herniation with cervical cord compression. C : Sagittal, T2-weighted MRI. D : Sagittal, cervical CT showed ossification of posterior longitudinal ligaments. E and F : Axial, T2-weighted, MRI scans showed excellent decompression after surgery. G : Sagittal T2-weighted, MRI scans. H : Posto-perative cervical 3D CT showed microforaminotomy hole at C4-5, C5-6, Rt.
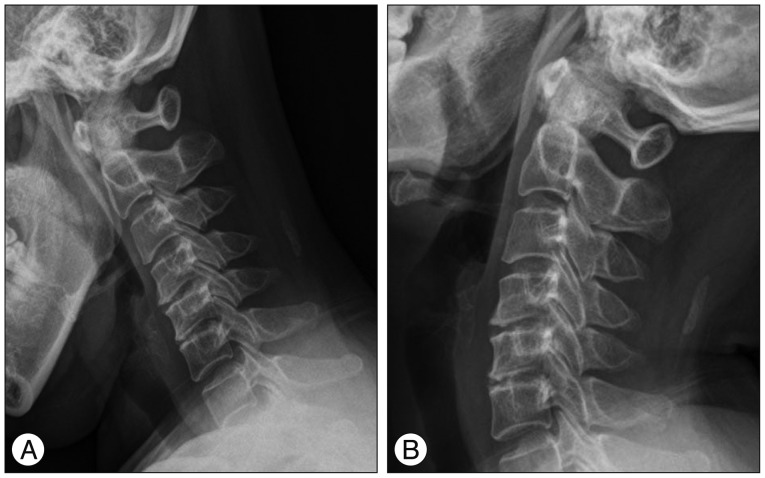
Fig. 3 Flexion (A) and extension (B) dynamic roentgenograms of the cervical spine, obtained 6 weeks after surgery, confirming normal motion at the C4-5, C5-6 level.
Reference
-
1. Batzdorf U, Batzdorff A. Analysis of cervical spine curvature in patients with cervical spondylosis. Neurosurgery. 1988; 22:827–836. PMID: 3380271.
Article2. Chacko AG, Joseph M, Turel MK, Prabhu K, Daniel RT, Jacob KS. Multilevel oblique corpectomy for cervical spondylotic myelopathy preserves segmental motion. Eur Spine J. 2012; 21:1360–1367. PMID: 22234720.
Article3. Chacko AG, Turel MK, Sarkar S, Prabhu K, Daniel RT. Clinical and radiological outcomes in 153 patients undergoing oblique corpectomy for cervical spondylotic myelopathy. Br J Neurosurg. 2014; 28:49–55. PMID: 23859056.
Article4. Chen TY, Crawford NR, Sonntag VK, Dickman CA. Biomechanical effects of progressive anterior cervical decompression. Spine (Phila Pa 1976). 2001; 26:6–13. discussion 14. PMID: 11148638.
Article5. Clarke E, Robinson PK. Cervical myelopathy : a complication of cervical spondylosis. Brain. 1956; 79:483–510. PMID: 13364095.
Article6. Hacker RJ, Miller CG. Failed anterior cervical foraminotomy. J Neurosurg. 2003; 98(2 Suppl):126–130. PMID: 12650395.
Article7. Haden N, Latimer M, Seeley HM, Laing RJ. Loss of inter-vertebral disc height after anterior cervical discectomy. Br J Neurosurg. 2005; 19:469–474. PMID: 16574558.
Article8. Jho HD. Decompression via microsurgical anterior foraminotomy for cervical spondylotic myelopathy. Technical note. J Neurosurg. 1997; 86:297–302. PMID: 9010435.
Article9. Jho HD, Kim MH, Kim WK. Anterior cervical microforaminotomy for spondylotic cervical myelopathy : part 2. Neurosurgery. 2002; 51(5 Suppl):S54–S59. PMID: 12234430.10. Jho HD, Kim WK, Kim MH. Anterior microforaminotomy for treatment of cervical radiculopathy : part 1--disc-preserving "functional cervical disc surgery". Neurosurgery. 2002; 51(5 Suppl):S46–S53. PMID: 12234429.11. Jung SS, Chung JC, Park KS, Chung SY, Park MS, Ha HG. Long-term follow-up results of anterior cervical microforaminotomy. Korean J Spine. 2010; 7:66–72.12. Kalsi-Ryan S, Karadimas SK, Fehlings MG. Cervical spondylotic myelopathy : the clinical phenomenon and the current pathobiology of an increasingly prevalent and devastating disorder. Neuroscientist. 2013; 19:409–421. PMID: 23204243.13. Kim JG, Kim SW, Lee SM, Shin H. Surgical result of the combined anterior and posterior approach in treatment of cervical spondylotic myelopathy. J Korean Neurosurg Soc. 2006; 3:188–191.14. Kim MH. Clinical and radiological long-term outcomes of anterior microforaminotomy for cervical degenerative disease. Spine (Phila Pa 1976). 2013; 38:1812–1819. PMID: 24150278.
Article15. Kim YG, Lee JS, Park MS, Ha HG. Midterm follow-up results of anterior cervical microforaminotomy. J Korean Neurosurg Soc. 2004; 35:250–255.16. Kotani Y, McNulty PS, Abumi K, Cunningham BW, Kaneda K, McAfee PC. The role of anteromedial foraminotomy and the uncovertebral joints in the stability of the cervical spine. A biomechanical study. Spine (Phila Pa 1976). 1998; 23:1559–1565. PMID: 9682312.
Article17. Lebl DR, Hughes A, Cammisa FP Jr, O'Leary PF. Cervical spondylotic myelopathy : pathophysiology, clinical presentation, and treatment. HSS J. 2011; 7:170–178. PMID: 22754419.
Article18. Oh SH, Perin NI, Cooper PR. Quantitative three-dimensional anatomy of the subaxial cervical spine : implication for anterior spinal surgery. Neurosurgery. 1996; 38:1139–1144. PMID: 8727144.
Article19. White AA 3rd, Johnson RM, Panjabi MM, Southwick WO. Biomechanical analysis of clinical stability in the cervical spine. Clin Orthop Relat Res. 1975; (109):85–96. PMID: 1132209.
Article20. Wu XD, Yuan W, Chen HJ, Chen Y, Wang JX, Cao P, et al. Neck motion following multilevel anterior cervical fusion : comparison of short-term and midterm results. J Neurosurg Spine. 2013; 18:362–366. PMID: 23373566.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Brown Sequard Syndrome Resulting from Cervical Disc Herniation Treated by Anterior Foraminotomy
- Endoscope Assisted Anterior Cervical Foraminotomy
- Posterior Endoscopic Cervical Discectomy
- Posterior Cervical Inclinatory Foraminotomy for Spondylotic Radiculopathy Preliminary
- Indirect Repair with Surgicel® and Fibrin Glue for Postoperative Cerebrospinal Fluid Leakage after Cervical Anterior Foraminotomy: A Case Report
