Nonfunctioning Parathyromatosis after Endoscopic Thyroid Lobectomy via an Axillo-Breast Approach: A Case Report
- Affiliations
-
- 1Department of Radiology, School of Medicine, Catholic University of Daegu, Daegu, Korea. jcpark@cu.ac.kr
- 2Department of Surgery, School of Medicine, Catholic University of Daegu, Daegu, Korea.
- KMID: 1941759
- DOI: http://doi.org/10.3348/jksr.2015.72.4.282
Abstract
- Parathyromatosis is characterized by multiple lesions of benign hyperfunctioning parathyroid tissue in the neck or mediastinum. Parathyromatosis is caused by proliferation of embryonic remnant or seeding of parathyroid tissue after parathyroidectomy. Parathyromatosis is rare but is the common cause of recurrent hyperparathyroidism. We describe a unique case of non-functional parathyromatosis in a 16-year-old girl with a history of right thyroid lobectomy via an axillo-breast approach for a nonfunctioning parathyroid adenoma in the right side of the neck.
MeSH Terms
Figure
-
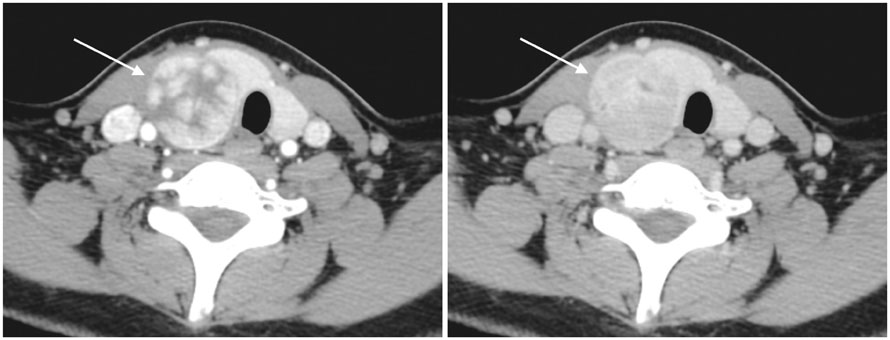
Fig. 1 Contrast-enhanced dynamic neck computed tomography showed early enhancing mass (arrow) with delayed wash-out in the posterior aspect of the right thyroid gland.

Fig. 2 A 16-year-old girl with parathyromatosis on ultrasonography. A. Ultrasonography of the anterior neck showed ovoid, homogeneous, and hypoechoic masses (arrows) at the superficial fatty layer of the anterior neck. B. Color Doppler ultrasonography revealed increased vascularity within the masses. Note.-Asterisk = vertebral body of cervical spine
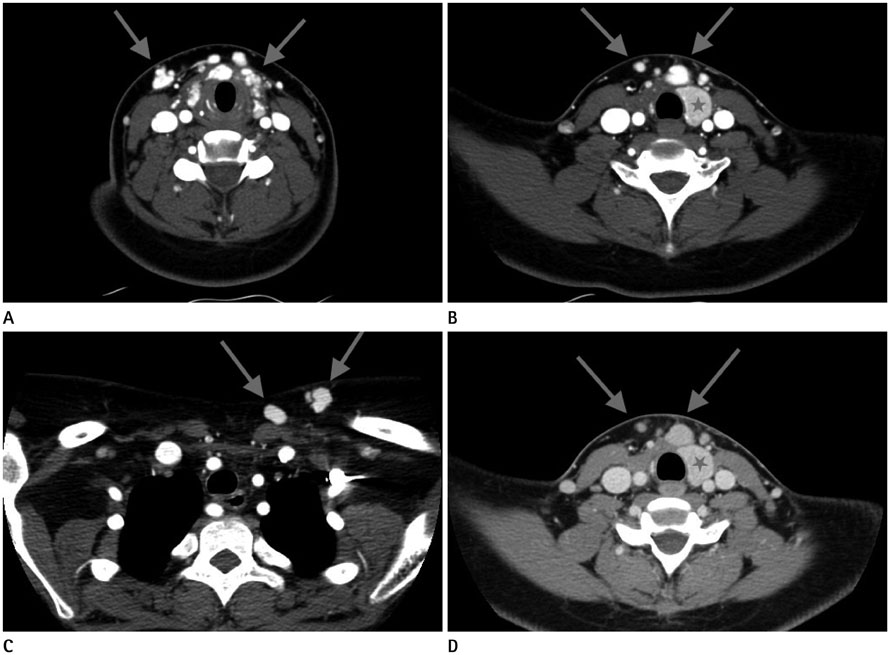
Fig. 3 A 16-year-old girl with parathyromatosis on contrast-enhanced dynamic neck CT. A-C. Contrast-enhanced dynamic neck computed tomography showed multiple lobulated early enhancing masses (arrows) at the right thyroid lobectomy site, anterior and posterior to strap musculature, and the subcutaneous layer of the anterior neck and left upper chest wall. D. These (arrows) were similarly dense compared to normal left thyroid lobe on delayed CT scan, measuring 2-15 mm in diameter. Note.-Asterisk = left thyroid gland
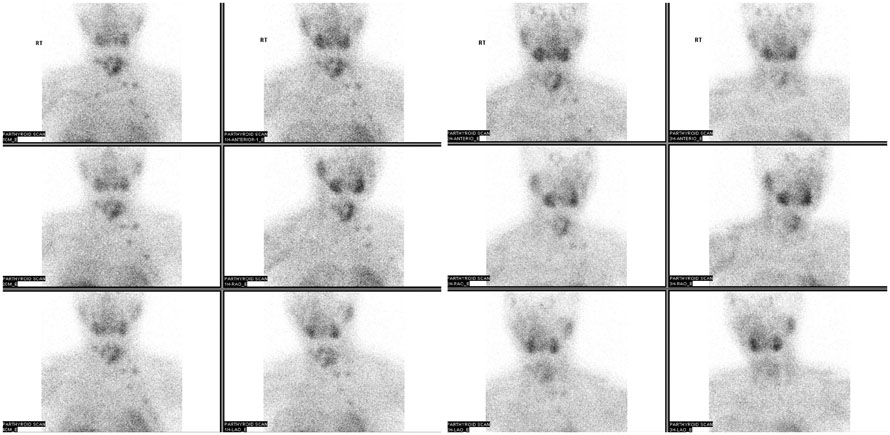
Fig. 4 Parathyroid scan showed delayed multiple tracer activities, suggesting parathyroid tissues in the anterior neck and upper chest wall.
Reference
-
1. Tublin ME, Yim JH, Carty SE. Recurrent hyperparathyroidism secondary to parathyromatosis: clinical and imaging findings. J Ultrasound Med. 2007; 26:847–851.2. Matsuoka S, Tominaga Y, Sato T, Uno N, Goto N, Katayama A, et al. Recurrent renal hyperparathyroidism caused by parathyromatosis. World J Surg. 2007; 31:299–305.3. Meakins JL, Milne CA, Hollomby DJ, Goltzman D. Total parathyroidectomy: parathyroid hormone levels and supernumerary glands in hemodialysis patients. Clin Invest Med. 1984; 7:21–25.4. Fernandez-Ranvier GG, Khanafshar E, Jensen K, Zarnegar R, Lee J, Kebebew E, et al. Parathyroid carcinoma, atypical parathyroid adenoma, or parathyromatosis? Cancer. 2007; 110:255–264.5. Palmer JA, Brown WA, Kerr WH, Rosen IB, Watters NA. The surgical aspects of hyperparathyroidism. Arch Surg. 1975; 110:1004–1007.6. Reddick RL, Costa JC, Marx SJ. Parathyroid hyperplasia and parathyromatosis. Lancet. 1977; 1:549.7. Rodgers SE, Hunter GJ, Hamberg LM, Schellingerhout D, Doherty DB, Ayers GD, et al. Improved preoperative planning for directed parathyroidectomy with 4-dimensional computed tomography. Surgery. 2006; 140:932–940. discussion 940-941.8. Miller DL, Craig WD, Haines GA. Retropharyngeal parathyroid adenoma: precise preoperative localization with CT and arterial infusion of contrast material. AJR Am J Roentgenol. 1997; 169:695–696.9. Randall GJ, Zald PB, Cohen JI, Hamilton BE. Contrast-enhanced MDCT characteristics of parathyroid adenomas. AJR Am J Roentgenol. 2009; 193:W139–W143.10. Beninato T, Kleiman DA, Scognamiglio T, Fahey TJ, Zarnegar R. Tract recurrence of a follicular thyroid neoplasm following transaxillary endoscopic thyroidectomy. Thyroid. 2012; 22:214–217.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral axillo-breast approach robotic total thyroidectomy without isthmectomy: a case report
- Endoscopic Thyroidectomy via an Axillo-bilateral Breast Approach: 5 Years of Experience
- Endoscopic Removal of Parathyroid Tumors via an Unilateral Axillo-Breast Approach
- A Clinical Analysis of Endoscopic Thyroid Lobectomy and Comparison with Conventional Thyroid Lobectomy
- A Clinical Analysis of Endoscopic Thyroidectomy via Bilateral Axillo-breast Approach: A 5-year Experience
