Bilateral Necrotizing Fasciitis around the Hips Differentiated from Fournier Gangrene: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, National Police Hospital, Seoul, Korea. ish0524@hanmail.net
- KMID: 1907706
- DOI: http://doi.org/10.5371/hp.2014.26.4.279
Abstract
- As an emergency encountered in orthopedic practice requiring prompt diagnosis and aggressive treatment, necrotizing fasciitis around the hip must be discriminated from Fournier gangrene. The current case report describes a patient who suffered from bilateral type I necrotizing fasciitis around the hips, which was alleviated by prompt surgical debridement and intensive postoperative care.
Keyword
MeSH Terms
Figure
-

Fig. 1 Initial plain radiography of the hip. Gas can be observed on the right gluteal area. The arrows indicate the margin of gas opacity.
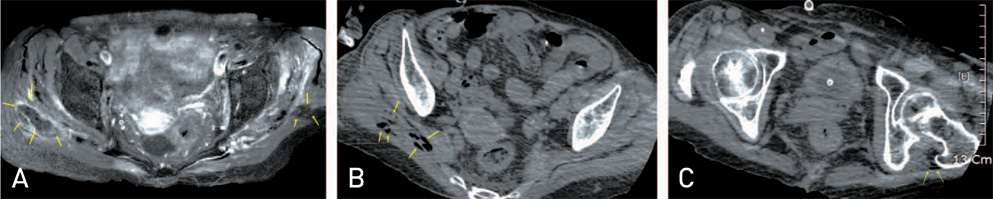
Fig. 2 Preoperative imaging studies. (A) A magnetic resonance image of the hip (axial view) shows abscess formation on the right side between the right gluteus maximus and the gluteus medius, and a smaller abscess on the left gluteus maximus. (B, C) Computed tomographic images of the hip (axial view) show gas tracking along the fascial planes on the right gluteal area (B) and on the left greater trochanteric area (C) only. The arrows indicate the margin of the abscess and gas.
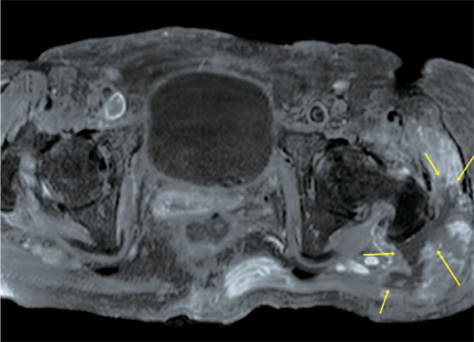
Fig. 3 Follow-up magnetic resonance image (MRI) of the hip. The size of the abscess around the left greater trochanter is increased in comparison to its size in the preoperative MRI (Fig. 2A). The arrows indicate the margin of the abscess.
Reference
-
1. Lee ST, Lee SH, Kim KM, Lee SJ. Necrotizing fasciitis of the low extremity. J Korean Orthop Assoc. 2005; 40:772–777.
Article2. Shaikh N. Necrotizing fasciitis: a decade of surgical intensive care experience. Indian J Crit Care Med. 2006; 10:225–229.
Article3. Machado NO. Necrotizing fasciitis: the importance of early diagnosis, prompt surgical debridement and adjuvant therapy. N Am J Med Sci. 2011; 3:107–118.
Article4. Song SJ, Lee IS, Chung JH. Type I, II acute necrotizing fasciitis of the low extremity. J Korean Orthop Assoc. 2007; 42:636–643.
Article5. Kim JO, Cho HM, Sin WJ, Bong HS. Necrotising fascitis of the thigh through short external rotator muscles due to an unrecognized perforated rectal cancer. Hip Pelvis. 2013; 25:149–152.
Article6. Elliott D, Kufera JA, Myers RA. The microbiology of necrotizing soft tissue infections. Am J Surg. 2000; 179:361–366.
Article7. Wysoki MG, Santora TA, Shah RM, Friedman AC. Necrotizing fasciitis: CT characteristics. Radiology. 1997; 203:859–863.
Article8. Wall DB, Klein SR, Black S, de Virgilio C. A simple model to help distinguish necrotizing fasciitis from nonnecrotizing soft tissue infection. J Am Coll Surg. 2000; 191:227–231.
Article9. Mallikarjuna MN, Vijayakumar A, Patil VS, Shivswamy BC. Fournier's gangrene: Current practices. ISRN Surg. 2012; 2012:942437.
Article10. Bilton BD, Zibari GB, McMillan RW, Aultman DF, Dunn G, McDonald JC. Aggressive surgical management of necrotizing fasciitis serves to decrease mortality: a retrospective study. Am Surg. 1998; 64:397–400. discussion 400-1.
