Successful Endovascular Aneurysm Repair for Abdominal Aortic Aneurysm in a Patient with Severe Coronary Artery Disease Undergoing Off-Pump Coronary Artery Bypass Grafting
- Affiliations
-
- 1Department of Cardiovascular Medicine, Chonnam National University Hospital, Gwangju, Korea. myungho@chollian.net
- KMID: 1889761
- DOI: http://doi.org/10.4068/cmj.2014.50.1.31
Abstract
- It is well known that patients with abdominal aortic aneurysm (AAA) often have concomitant coronary artery disease (CAD). In cases of AAA with severe CAD requiring coronary artery bypass grafting (CABG), two therapeutic strategies regarding the timing of CABG can be considered: staged or simultaneous operations. However, the ideal treatment of patients with large AAA and critical CAD remains controversial. We experienced a case of successful endovascular aneurysm repair after off-pump CABG in a 70-year-old patient who had a huge AAA and critical CAD.
MeSH Terms
Figure
-

FIG. 1 Electrocardiography showed sinus rhythm with first-degree atrioventricular block, left atrial enlargement, and left bundle branch block.

FIG. 2 Two-dimensional echocardiographic findings. Marked dilation of the LV chamber with severe LV systolic dysfunction (A) and a huge apical thrombus (B). Severe MR with PISA radius of 0.99 cm (C) and EROA of 0.5 cm2 (D). LV: left ventricle, MR: mitral regurgitation, PISA: proximal isovelocity surface area, EROA: effective regurgitant orifice area.

FIG. 3 Ultrasonographic and CT findings of AAA. A 76-mm abdominal aortic aneurysm with thrombosed false lumen shown by abdominal ultrasonography (A). Aneurysmal dilatation of the infra-renal abdominal aorta (B) and both thrombosed common iliac arteries (C) shown by CT angiography. Three-dimensional reconstructed image demonstrating aneurysmal dilatation infra-renal abdominal aorta extending to both the common and internal iliac arteries (D). AAA: abdominal aortic aneurysm, CT: computed tomography.
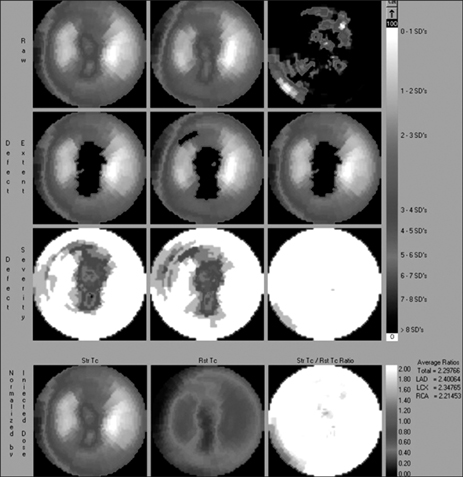
FIG. 4 Tc-99m MIBI myocardial SPECT showing fixed perfusion defect in the apex, anterior wall, and inferior wall. Tc-99m MIBI: technetium-99m methoxyisobutylisonitrile, SPECT: single-proton emission computed tomography.

FIG. 5 Aortographic and coronary angiographic findings. Huge infra-renal abdominal aneurysm shown by aortogram (A). Near total occlusion in mLAD and critical stenosis in LCx-os (B) with collateral flow to RCA (C) and total occlusion in dRCA, visualized only by nonselective ascending aortogram due to its anomalous origin (D). mLAD: middle left anterior descending artery, LCx-os: ostium of the left circumflex artery, dRCA: distal right coronary artery.
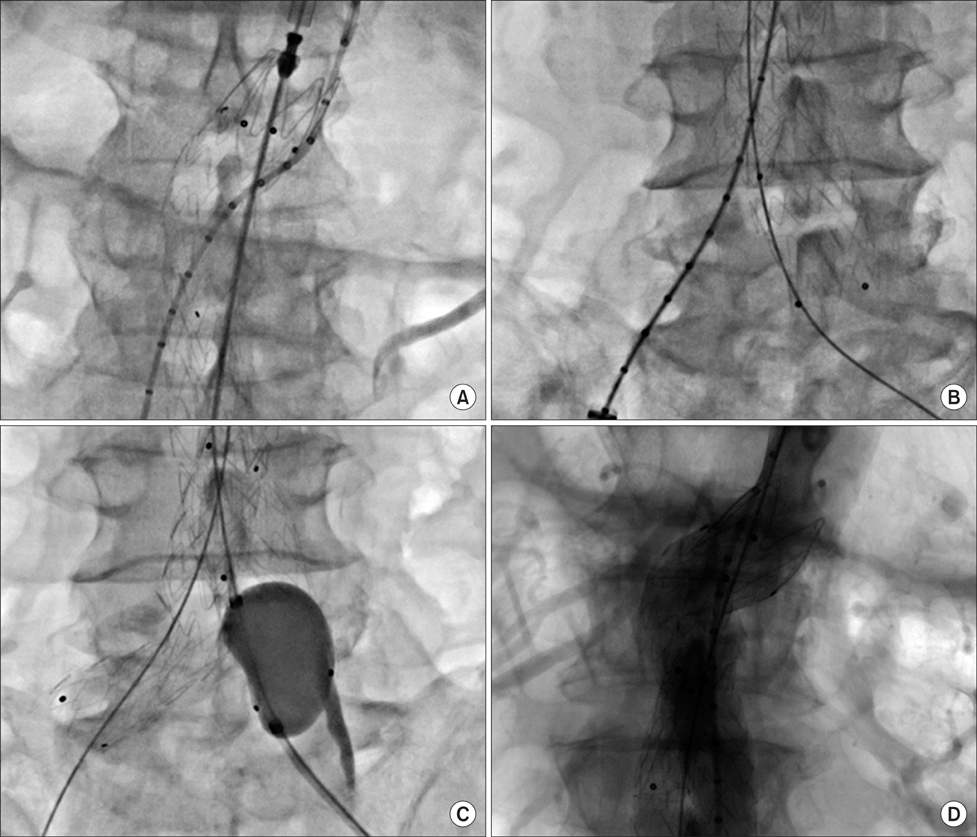
FIG. 6 Endovascular aneurysm repair (EVAR) findings. Implantation of a main body graft stent (A) and deployment of stent for the right common iliac artery (B). Stent expansion to its distal end using a balloon (C). Good expansion of the stents without any leakage (D).
Reference
-
1. Jang MO, Kim JH, Oh SK, Lee MG, Park KH, Sim DS, et al. Endovascular stent in traumatic thoracic aortic dissection. Korean Circ J. 2012; 42:341–344.
Article2. Giles KA, Pomposelli F, Hamdan A, Wyers M, Jhaveri A, Schermerhorn ML. Decrease in total aneurysm-related deaths in the era of endovascular aneurysm repair. J Vasc Surg. 2009; 49:543–550.
Article3. Chaikof EL, Brewster DC, Dalman RL, Makaroun MS, Illig KA, Sicard GA, et al. The care of patients with an abdominal aortic aneurysm: the Society for Vascular Surgery practice guidelines. J Vasc Surg. 2009; 50:4 Suppl. S2–S49.
Article4. Moll FL, Powell JT, Fraedrich G, Verzini F, Haulon S, Waltham M, et al. Management of abdominal aortic aneurysms clinical practice guidelines of the European society for vascular surgery. Eur J Vasc Endovasc Surg. 2011; 41:Suppl 1. S1–S58.
Article5. Hertzer NR, Beven EG, Young JR, O'Hara PJ, Ruschhaupt WF 3rd, Graor RA, et al. Coronary artery disease in peripheral vascular patients. A classification of 1000 coronary angiograms and results of surgical management. Ann Surg. 1984; 199:223–233.6. Cuypers PW, Gardien M, Buth J, Peels CH, Charbon JA, Hop WC. Randomized study comparing cardiac response in endovascular and open abdominal aortic aneurysm repair. Br J Surg. 2001; 88:1059–1065.
Article7. Paty PS, Darling RC 3rd, Chang BB, Lloyd WE, Kreienberg PB, Shah DM. Repair of large abdominal aortic aneurysm should be performed early after coronary artery bypass surgery. J Vasc Surg. 2000; 31:253–259.
Article8. de la Motte L, Jensen LP, Vogt K, Kehlet H, Schroeder TV, Lonn L. Outcomes after elective aortic aneurysm repair: a nationwide Danish cohort study 2007-2010. Eur J Vasc Endovasc Surg. 2013; 46:57–64.
Article9. Morimoto K, Taniguchi I, Miyasaka S, Suda T, Yamaga T, Sakamoto M, et al. Combined coronary artery bypass grafting on the beating heart and abdominal aortic aneurysm repair. Circ J. 2002; 66:755–757.
Article10. Wolff T, Baykut D, Zerkowski HR, Stierli P, Gürke L. Combined abdominal aortic aneurysm repair and coronary artery bypass: presentation of 13 cases and review of the literature. Ann Vasc Surg. 2006; 20:23–29.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Wrapping of an Ascending Aortic Aneurysm with the Multiple Boot-Straps Technique in a Patient Undergoing Off-Pump Coronary Artery Bypass Grafting
- Endovascular aortic aneurysm repair using a bifurcated stent graft in a patient with femoro-femoral bypass
- Anesthesia for Off-pump Coronary Artery Bypass Grafting Surgery in a Child with Coronary Disease due to Kawasaki Disease
- EVAR with Hypogastric Artery Bypass in Patient with Abdominal Aorto-Iliac Aneurysm
- Cardiac Arrest after Aortic Cross Clamping during Surgery for an Abdominal Aortic Aneurysm in a Patient with Coronary Artery Disease and Aortic Regurgitation: A Case Report
