Successful laparoscopic reversal of gastric bypass in a patient with malnutrition
- Affiliations
-
- 1Department of Surgery, Soonchunhyang University Seoul Hospital, Seoul, Korea. yjgs1997@gmail.com
- KMID: 1882829
- DOI: http://doi.org/10.4174/astr.2014.87.4.217
Abstract
- Roux-en-Y gastric bypass (RYGB) is one of the most commonly performed bariatric procedures around the world. Although RYGB is the gold standard for treating morbid obesity, it carries the risk of rare but serious long-term complications from malnutrition. We report a case of laparoscopic reversal of RYGB. A female patient reported prolonged incapacitating postprandial pain that consequently made her avoid proper oral intake. Therefore, she became seriously malnourished at 30 months after RYGB and requested reversal of RYGB into normal anatomy. The operation was successfully performed via laparoscopy. Operating time was 120 minutes, and intraoperative blood loss was 20 mL. The patient was discharged without any complications directly related to surgical procedures, although her hospital stay was prolonged by the treatment of asymptomatic septicemia of unknown origin. Laparoscopic reversal of RYGB into normal anatomy is technically feasible and might be performed safely after thorough preoperative evaluation in carefully selected patients.
MeSH Terms
Figure
-

Fig. 1 Details of the Roux-en-Y gastric bypass reversal. (A) Division of the alimentary limb right below the old gastrojejunostomy. (B) Transection of the gastrojejunostomy near the distal end of the gastric pouch. (C) Construction of the gastrogastric anastomosis between the gastric pouch remnant and excluded stomach using a linear stapler. (D) Newly established gastrogastrostomy (red arrows). (E) Entero-entero anastomosis between the proximal end of the old alimentary limb and the distal end of the old biliopancreatic limb. (F) Newly established enteroenterostomy.
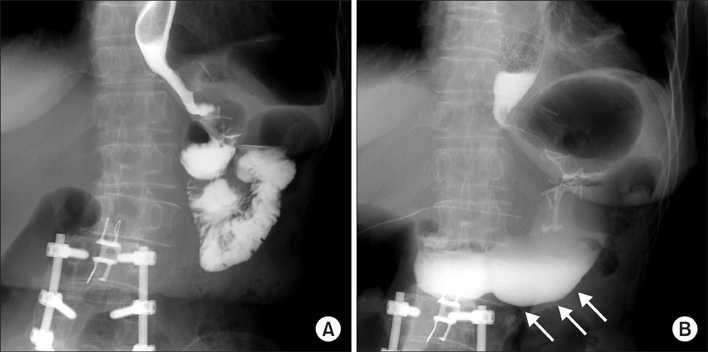
Fig. 2 Pre- and postoperative contrast upper gastrointestinal (UGI) studies. (A) UGI image before the reversal of the Roux-en-Y gastric bypass (RYGB). (B) UGI image after the RYGB reversal. Contrast passage into the old excluded stomach is noted after the reversal operation (white arrows).
Reference
-
1. Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004; 292:1724–1737.2. Himpens J, Dapri G, Cadiere GB. Laparoscopic conversion of the gastric bypass into a normal anatomy. Obes Surg. 2006; 16:908–912.3. Vilallonga R, van de Vrande S, Himpens J. Laparoscopic reversal of Roux-en-Y gastric bypass into normal anatomy with or without sleeve gastrectomy. Surg Endosc. 2013; 27:4640–4648.4. Dapri G, Cadiere GB, Himpens J. Laparoscopic reconversion of Roux-en-Y gastric bypass to original anatomy: technique and preliminary outcomes. Obes Surg. 2011; 21:1289–1295.5. Poitou Bernert C, Ciangura C, Coupaye M, Czernichow S, Bouillot JL, Basdevant A. Nutritional deficiency after gastric bypass: diagnosis, prevention and treatment. Diabetes Metab. 2007; 33:13–24.6. Allied Health Sciences Section Ad Hoc Nutrition Committee. Aills L, Blankenship J, Buffington C, Furtado M, Parrott J. ASMBS Allied Health Nutritional Guidelines for the surgical weight loss patient. Surg Obes Relat Dis. 2008; 4:5 Suppl. S73–S108.7. Dalcanale L, Oliveira CP, Faintuch J, Nogueira MA, Rondo P, Lima VM, et al. Long-term nutritional outcome after gastric bypass. Obes Surg. 2010; 20:181–187.8. Kellum JM, Chikunguwo SM, Maher JW, Wolfe LG, Sugerman HJ. Long-term results of malabsorptive distal Roux-en-Y gastric bypass in superobese patients. Surg Obes Relat Dis. 2011; 7:189–193.9. Skroubis G, Sakellaropoulos G, Pouggouras K, Mead N, Nikiforidis G, Kalfarentzos F. Comparison of nutritional deficiencies after Roux-en-Y gastric bypass and after biliopancreatic diversion with Roux-en-Y gastric bypass. Obes Surg. 2002; 12:551–558.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous gastrostomy tube placement of the excluded gastric remnant after laparoscopic bariatric surgery in three patients
- Laparoscopic Hiatal Hernia Repair during Laparoscopic Roux-en-Y Gastric Bypass (LRYGB)
- Heparin Anticoagulation and Natural Reversal in a Patient with Anaphylactoid Shock to Protamine: A case report
- Conversion of One-Anastomosis Gastric Bypass (OAGB) to Roux-en-Y Gastric Bypass (RYGB) is Effective in Dealing with Late Complications of OAGB: Experience from a Tertiary Bariatric Center and Literature Review
- A case of bypass arthritis-dermatitis syndrome after bypass gastrojejunostomy
