Mesoesophagus and other fascial structures of the abdominal and lower thoracic esophagus: a histological study using human embryos and fetuses
- Affiliations
-
- 1Department of Surgery, Daejeon Sun Hospital, Daejeon, Korea.
- 2Department of Anatomy, Chonbuk National University Medical School, Jeonju, Korea. 407kk@hanmail.net
- 3Department of Surgery and Biomedical Research Institute, Chonbuk National University Hospital, Jeonju, Korea.
- 4Institute of Embryology, Universitad Complutense, Madrid, Spain.
- 5Division of Internal Medicine, Iwamizawa Asuka Hospital, Iwamizawa, Japan.
- KMID: 1882601
- DOI: http://doi.org/10.5115/acb.2014.47.4.227
Abstract
- A term "mesoesophagus" has been often used by surgeons, but the morphology was not described well. To better understand the structures attaching the human abdominal and lower thoracic esophagus to the body wall, we examined serial or semiserial sections from 10 embryos and 9 fetuses. The esophagus was initially embedded in a large posterior mesenchymal tissue, which included the vertebral column and aorta. Below the tracheal bifurcation at the fifth week, the esophagus formed a mesentery-like structure, which we call the "mesoesophagus," that was sculpted by the enlarging lungs and pleural cavity. The pneumatoenteric recess of the pleuroperitoneal canal was observed in the lowest part of the mesoesophagus. At the seventh week, the mesoesophagus was divided into the upper long and lower short parts by the diaphragm. Near the esophageal hiatus, the pleural cavity provided 1 or 2 recesses in the upper side, while the fetal adrenal gland in the left side was attached to the lower side of the mesoesophagus. At the 10th and 18th week, the mesoesophagus remained along the lower thoracic esophagus, but the abdominal esophagus attached to the diaphragm instead of to the left adrenal. The mesoesophagus did not contain any blood vessels from the aorta and to the azygos vein. The posterior attachment of the abdominal esophagus seemed to develop to the major part of the phrenoesophageal membrane with modification from the increased mass of the left fetal adrenal. After postnatal degeneration of the fetal adrenal, the abdominal esophagus might again obtain a mesentery. Consequently, the mesoesophagus seemed to correspond to a small area containing the pulmonary ligament and aorta in adults.
MeSH Terms
Figure
-
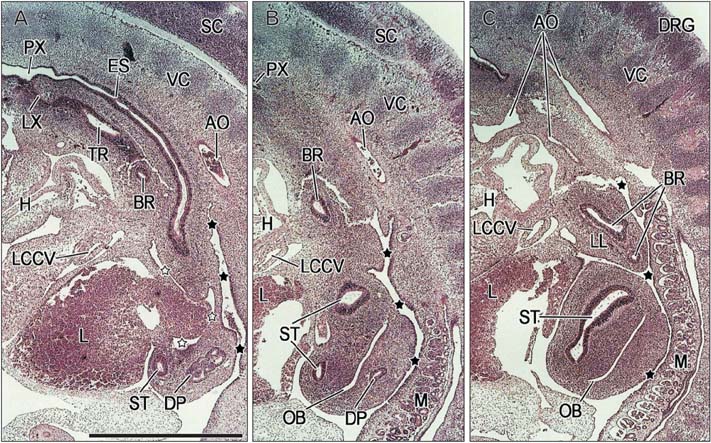
Fig. 1 Sagittal sections of a 10-mm crown-rump length embryo (approximately 5 weeks). Panels (A) and (C) are the right- and left-most sides of the figure, respectively. Intervals between panels are 0.1 mm. Panel (A) displays an almost entire course of the esophagus (ES). The esophagus and aorta (AO) are embedded in posterior mesenchymal tissue continuous with the vertebral column. (B) Since the tracheal bifurcation almost corresponds to the caption bronchus (BR), a short distance between the bifurcation and stomach is evident. (C) The stomach is just below the left lung (LL) and is separated from the liver (L) and mesonephros (M) by a peritoneal recess (black stars). The space with open stars corresponds to the future superior recess of the omental bursa (OB). The major part of the OB starts to develop in the dorsal mesogastrium (B, C). AO in panel (C) indicates the left- and right-sided aortas as well as the fourth pharyngeal arch artery. DP, dorsal pancreas; DRG, dorsal root ganglia; H, heart; LCCV, left common cardinal vein; LX, larynx; PX, pharynx; SC, spinal cord; ST, stomach; TR, trachea; VC, vertebral column. All panels were prepared at the same magnification. Scale bar=1 mm.
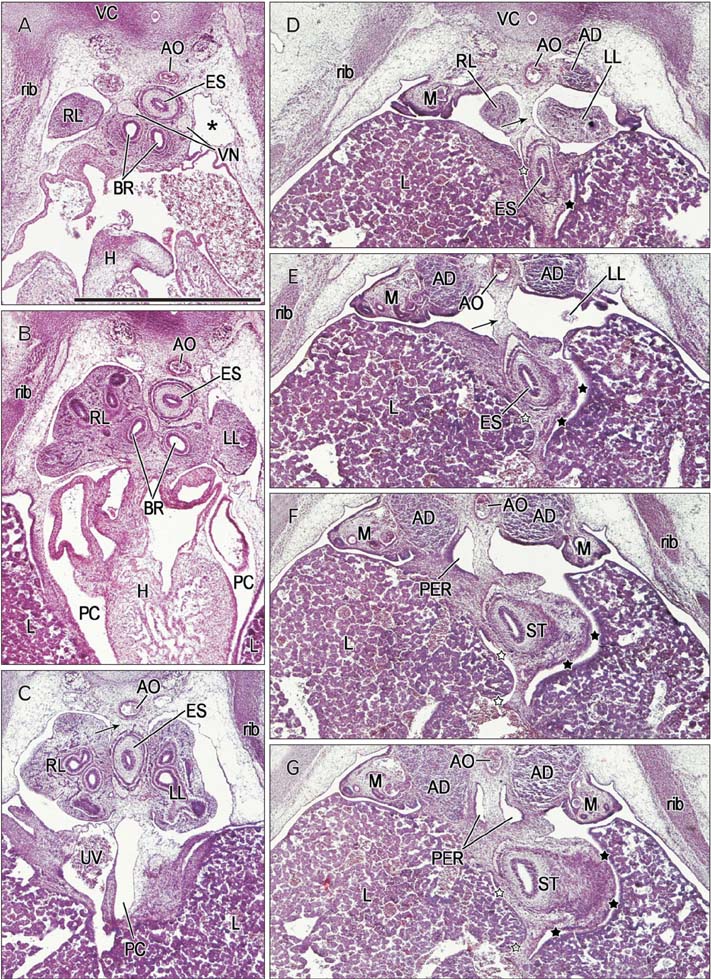
Fig. 2 Horizontal sections of a 13-mm crown-rump leng th embr yo (approximately 5 weeks). Panels (A) and (G) are the most superior and inferior sides of the figure, respectively. Intervals between panels are 0.1 mm (A, B), 0.4 mm (B, C), 0.2 mm (C, D) and 0.1 mm (D-G). Panels (A) and (B) show levels immediately below the tracheal bifurcation: the esophagus (ES) is located on the anterior side of the aorta (AO). The asterisk in panel (A) indicates the apex of the pleural cavity. The umbilical vein (UV) runs upward along the inferior part of the pericardium (C). The diaphragm has not yet developed and the pleural and peritoneal cavities communicate via the pleuroperitoneal canal. Thus, in panel (D), the left lung (LL) faces the adrenal (AD) and liver (L) without interrupting any membranous structure. (C-E) The esophagus is connected with the aorta by a mesentery-like structure (i.e., the mesoesophagus; arrow). The pneumatoenteric recesses (PER; recesses of the pleuroperitoneal canal) are present at the inferior end of the mesoesophagus (F, G). The stomach (ST) is separated from the liver (L) by peritoneal recesses (black stars in panels D-G): and by the future omental bursa (OB, open stars). A terminal portion of the UV does not simply correspond to the inferior vena cava due to a lack of communication with the adrenal vein [5]. BR, bronchus; H, heart; M, mesonephros; PC, pericardial cavity; RL, right lung ; ST, stomach; VC, vertebral column; VN, vagus nerve. All panels were prepared at the same magnification. Scale bar=1 mm.
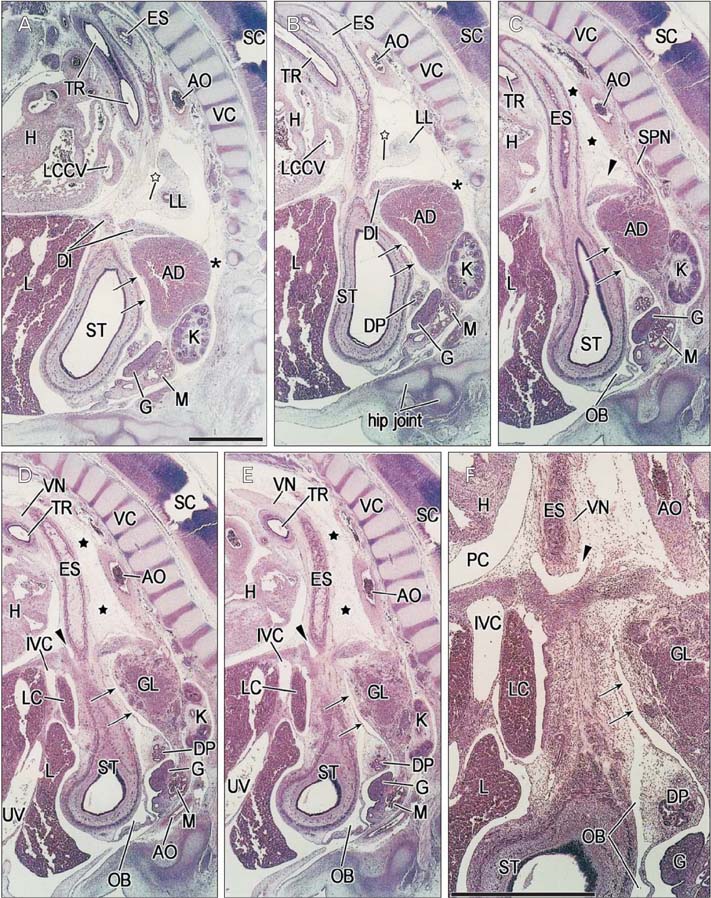
Fig. 3 Sag ittal sections of a 22-mm crown-rump leng th embr yo (approximately 7 weeks). Panels (A) and (F) are the left- and right-most sides of the figure, respectively. Intervals between panels are 0.1 mm (A, B), 0.3 mm (B, C) and 0.1 mm (C-F). Panels (A-E) were prepared at the same magnification, while panel (F) is at a higher magnification to show details of the fascia and space. Scale bar=1 mm. Panels (A) and (B) contain the right end of the left lung (LL), which is connected to the esophagus (ES) by a mesentery-like structure (open stars). In panel (C), the loose mesenchymal tissue (black stars) between the esophagus and aorta (AO) corresponds to the mesoesophagus. A recess of the peritoneal cavity (arrows) separates the stomach (ST) and abdominal esophagus from the adrenal (AD) and celiac ganglion (GL). The diaphragm (DI) has not yet extended to the space behind the AD (asterisks in panels A and B). At the superior aspect of the diaphragm, the esophagus is surrounded by a recess of the pleural cavity (arrowheads in panels C-F). The liver caudate lobe (LC) protrudes into the omental bursa (OB) in panels (D-F). DP, dorsal pancreas; G, gonad; H, heart; IVC, inferior vena cava; K, kidney; L, liver; LCCV, left common cardinal vein; M, mesonephros; PC, pericardial cavity; SC, spinal cord; SPN, splanchnic nerve; TR, trachea; UV, umbilical vein; VC, vertebral column; VN, vagus nerve.
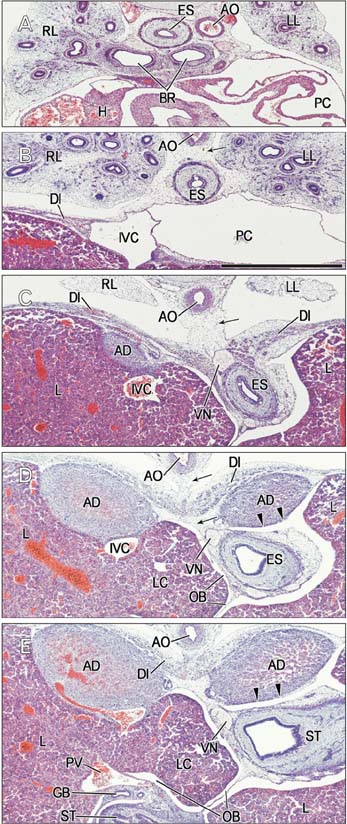
Fig. 4 Horizontal sections of a 22-mm crown-rump length embryo (approximately 7 weeks). Panels (A) and (E) are the most superior and inferior sides of the figure, respectively. The intervals between panels are 0.9 mm (A, B), 0.8 mm (B, C), 0.2 mm (C, D), and 0.1 mm (D, E). Panel (A) shows a level immediately below the tracheal bifurcation, with the esophagus (ES) located on the right side of the aorta (AO). In panels (B) and (C), the esophagus is connected with the aorta by the mesoesophagus (arrows). However, in panel (D), the mesoesophagus (arrows) is interrupted by the diaphragm. In panels (D) and (E), the adrenal (AD) is separated from the stomach (ST) or abdominal esophagus by a recess of the peritoneal cavity (arrowheads). The liver caudate lobe (LC) protrudes into the omental bursa (OB). BR, bronchus; DI, diaphragm; ES, esophagus; GB, gallbladder; H, heart; IVC, inferior vena cava; L, liver; LL, left lung; PC, pericardial cavity; PV, portal vein; RL, right lung; VN, vagus nerve. All panels were prepared at the same magnification. Scale bar=1 mm.
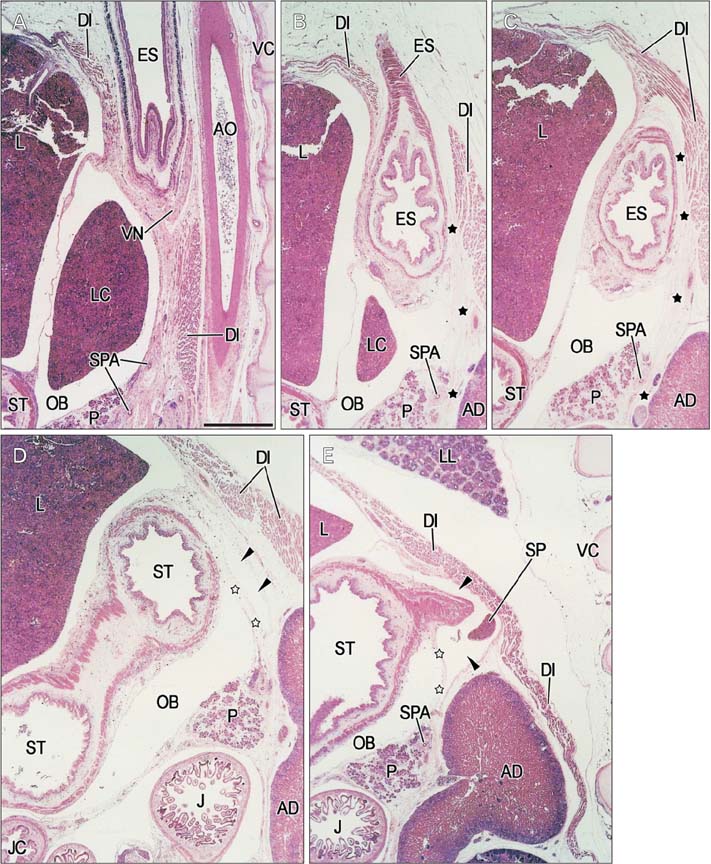
Fig. 5 Sagittal sections of a 56-mm crown-rump leng th fetus (approximately 10 weeks). Panels (A) and (E) are the right- and left-most sides of the figure, respectively. Intervals between panels are 1.1 mm (A, B), 0.3 mm (B, C), 0.9 mm (C, D), and 0.1 mm (D, E). In panels (A) and (B), the liver caudate lobe (LC) protrudes into the omental bursa (OB). In panels (B) and (C), the esophagus is attached to the abdominal aspect of the diaphragm (DI); the interface contains a fascia (black stars) that appears to extend downward between the pancreas (P) and adrenal (AD). In panels (D) and (E), a recess of the peritoneal cavity (arrowheads) is surrounded by the AD, the stomach and the dorsal mesogastrium (open stars). AD, adrenal gland (fetal adrenal cortex); AO, aorta; ES, esophagus; J, jejunum; L, liver; LL, left lung ; OB, omental bursa; P, pancreas; SP, spleen; SPA, splenic artery; ST, stomach; TC, transverse colon; VC, vertebral column; VN, vagus ner ve. All panels were prepared at the same magnification. Scale bar=1 mm.
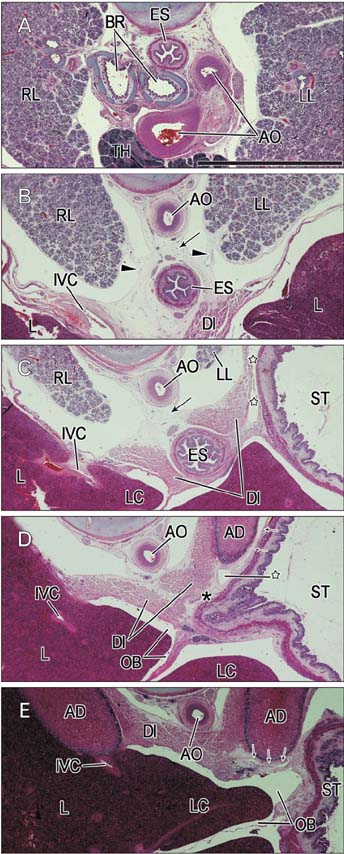
Fig. 6 Tilted horizontal sections of a 155-mm crown-rump length fetus (approximately 18 weeks). Panels (A) and (E) are the most superior and inferior sides of the figure, respectively. Intervals between panels are 16.5 mm (A, B), 2.8 mm (B, C), 2.4 mm (C, D), and 1.6 mm (D, E). Panel (A) shows a level immediately below the tracheal bifurcation, with the esophagus (ES) located on the right side of the aorta (AO). In panels (B) and (C), the mesoesophagus (arrows) connects the aorta and esophagus. Arrowheads in panel (B) indicate bilateral recesses of the pleural cavity in the pulmonary ligament. The abdominal esophagus is attached to the diaphragm (asterisk in panel D). A recess of the peritoneal cavity (open stars in panel C), present between the stomach and left adrenal, provides a sac-like enlargement (open star in panel D). Another slit-like recess is also seen (arrows in panels D and E). The liver caudate lobe (LC) protrudes into the omental bursa (OB). AD, adrenal gland (fetal adrenal cortex); BR, bronchus; DI, diaphragm; IVC, inferior vena cava; L, liver; LC, liver caudate lobe; LL, left lung; RL, right lung; ST, stomach; TH, thymus. All panels were prepared at the same magnification. Scale bar=1 mm.
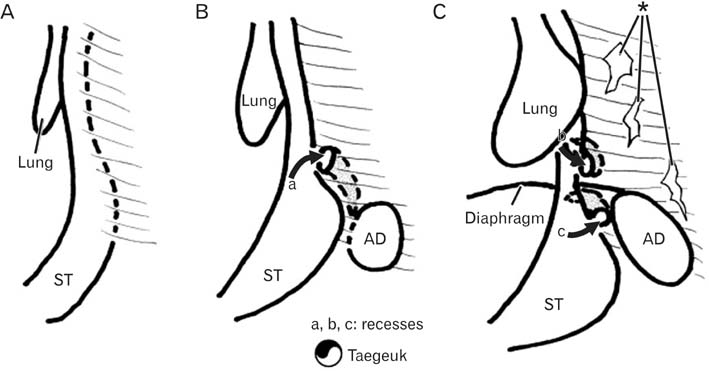
Fig. 7 A schematic representation showing recesses of the celomic, pleural and peritoneal cavities protruding into the mesoesophagus. Panel (A) (at and before 5 weeks) exhibits a primitive form in which the esophagus is embedded in a posterior mesenchymal tissue. Panel (B) (5 weeks) displays an initial mesoesophagus with the pneumatoenteric recess (a curved arrow with a): the mesentery-like shape is sculptured by the developing lungs. Panel (C) (7-18 weeks) shows a pleural recess around the lower thoracic esophagus (a curved arrow with b) as well as a peritoneal recess behind the abdominal esophagus (a curved arrow with c) between the left adrenal (AD) and stomach (ST). Asterisk indicates disappearance of the posterior mesenchymal tissue, including the mesoesophagus, due to cell death. Those recesses are similar to a Korean traditional symbol of the nature in shape, i.e., Taegeuk, as shown in the lower part of the figure.
Reference
-
1. Hamilton WJ, Mossman HW. Human embryology: prenatal development of form and function. 4th ed. Lodon: Williams & Wilkins;1978. p. 334–337.2. Hayashi S, Fukuzawa Y, Rodríguez-Vázquez JF, Cho BH, Verdugo-López S, Murakami G, Nakano T. Pleuroperitoneal canal closure and the fetal adrenal gland. Anat Rec (Hoboken). 2011; 294:633–644.3. Jin ZW, Nakamura T, Yu HC, Kimura W, Murakami G, Cho BH. Fetal anatomy of peripheral lymphatic vessels: a D2-40 immunohistochemical study using an 18-week human fetus (CRL 155 mm). J Anat. 2010; 216:671–682.4. Kanagasuntheram R. Development of the human lesser sac. J Anat. 1957; 91:188–206.5. Jin ZW, Cho BH, Murakami G, Fujimiya M, Kimura W, Yu HC. Fetal development of the retrohepatic inferior vena cava and accessory hepatic veins: Re-evaluation of the Alexander Barry's hypothesis. Clin Anat. 2010; 23:297–303.6. Yang JD, Ishikawa K, Hwang HP, Yu HC, Rodríguez-Vázquez JF, Murakami G, Cho BH. Morphology of the ligament of Treitz likely depends on its fetal topographical relationship with the left adrenal gland and liver caudate lobe as well as the developing lymphatic tissues: a histological study using human fetuses. Surg Radiol Anat. 2013; 35:25–38.7. Perlemuter L, Waligora J. Cahiers d'anatomie. Vol. 6. Thorax. 3rd ed. Paris: Masson;1976.8. Miyake N, Takeuchi H, Cho BH, Murakami G, Fujimiya M, Kitano H. Fetal anatomy of the lower cervical and upper thoracic fasciae with special reference to the prevertebral fascial structures including the suprapleural membrane. Clin Anat. 2011; 24:607–618.9. Boutelier P, Lefort R. Anatomic study of the abdominal mesoesophagus. Surgical deductions. J Chir (Paris). 1970; 100:371–384.10. Cho BH, Kimura W, Song CH, Fujimiya M, Murakami G. An investigation of the embryologic development of the fascia used as the basis for pancreaticoduodenal mobilization. J Hepatobiliary Pancreat Surg. 2009; 16:824–831.11. Hayashi S, Murakami G, Ohtsuka A, Itoh M, Nakano T, Fukuzawa Y. Connective tissue configuration in the human liver hilar region with special reference to the liver capsule and vascular sheath. J Hepatobiliary Pancreat Surg. 2008; 15:640–647.12. Yang JD, Ishikawa K, Hwang HP, Park DE, Song JS, Fujimiya M, Murakami G, Cho BH. Retropancreatic fascia is absent along the pancreas facing the superior mesenteric artery: a histological study using elderly donated cadavers. Surg Radiol Anat. 2013; 35:403–410.13. Watanabe Y, Lister J. Development of the human fetal phrenoesophageal membrane and its role in the anti-reflux mechanism. Surg Today. 1993; 23:722–727.14. Kinoshita H, Umezawa T, Omine Y, Kasahara M, Rodríguez-Vázquez JF, Murakami G, Abe S. Distribution of elastic fibers in the head and neck: a histological study using late-stage human fetuses. Anat Cell Biol. 2013; 46:39–48.15. St Peter SD, Barnhart DC, Ostlie DJ, Tsao K, Leys CM, Sharp SW, Bartle D, Morgan T, Harmon CM, Georgeson KE, Holcomb GW 3rd. Minimal vs extensive esophageal mobilization during laparoscopic fundoplication: a prospective randomized trial. J Pediatr Surg. 2011; 46:163–168.16. Kwok H, Mariz Y, Al-Ali S, Windsor JA. Phrenoesophageal ligament re-visited. Clin Anat. 1999; 12:164–170.17. Apaydin N, Uz A, Evirgen O, Loukas M, Tubbs RS, Elhan A. The phrenico-esophageal ligament: an anatomical study. Surg Radiol Anat. 2008; 30:29–36.18. Nakajima F, Murakami G, Ohyama S, Horiguchi T, Sakakura Y, Yajima T, Hirata K. Potential fascial dome made by the upper leaf of the phreno-esophageal membrane. Okajimas Folia Anat Jpn. 2001; 77:201–209.19. Okabayashi T, Kobayashi M, Sucgimoto T, Ohara S, Okamoto K, Matsuura K, Araki K. Posterior gastric artery in angiograms and its surgical importance. Hepatogastroenterology. 2005; 52:298–301.20. Hwang SE, Cho BH, Hirai I, Kim HT, Kim JH, Fujimiya M, Murakami G, Kimura W. Topographical anatomy of Spiegel’s lobe and its adjacent organs in mid-term fetuses: its implication on the development of the lesser sac and adult morphology of the upper abdomen. Clin Anat. 2010; 23:712–719.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intestinal Rotation, Luminal Obstruction and Recanalization in the Human Embryos and Fetuses
- Persistent right umbilical vein: a study using serial sections of human embryos and fetuses
- Histological Observations on Human Thyroids: 100 cases analysis of embryos and fetuses
- A Case of Intra-Abdominal Esophageal Duplication Cyst
- Development of the Shoulder Joint in Staged Human Embryos and Fetuses in Korean
