Giant Cell-Rich Osteosarcoma: A Tumor Simulating Borderline Lesion
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea Cancer Center Hospital, Seoul, Korea. dgjeon@kirams.re.kr
- 2Department of Pathology, Korea Cancer Center Hospital, Seoul, Korea.
- KMID: 1851956
- DOI: http://doi.org/10.4055/jkoa.2015.50.3.225
Abstract
- PURPOSE
Giantcell-rich osteosarcoma (GCRO) is a rare subtype of osteosarcoma. We reviewed; 1) radiological finding of GCRO and clinical impression-related diagnostic workup at referral center, 2) diagnostic delay until a proper diagnosis is made, 3) impact of diagnostic delay on the oncologic outcome.
MATERIALS AND METHODS
We reviewed 17 patients with GCRO. We investigated the plain radiographic finding, tumor size and location, presence of pathologic fracture, clinical impression and pathological diagnosis at referral center, diagnostic delay, definitive treatment, local recurrence, metastasis, and survival rate.
RESULTS
Eleven cases (64.7%) showed a plain radiographically, purely osteolytic pattern while 6 cases (35.3%) showed mixed osteolytic and sclerotic lesion. Diagnosis at primary center was osteosarcoma in 7 (41.2%), giant cell tumor in 7 (41.2%), and benign bone tumor in 3 (17.6%). Six patients (35.3%) experienced diagnostic delay. Mean diagnostic delay was 3.1 months (1 to 8). At final follow-up 5-year actuarial survival rate of 17 patients was 65%+/-25%. Although 11 patients without diagnostic delay showed a tendency of high survival over 6 patients with diagnostic problem, there was no statistical significance (p=0.14).
CONCLUSION
GCRO is a rare subtype of osteosarcoma simulating giant cell tumor both pathologically and radiologically. Careful diagnostic approach is required in order not to misdiagnose this malignant tumor.
MeSH Terms
Figure
-

Figure 1 Plain radiograph of a 13-year-old female shows a mixed osteolytic and sclerotic lesion in the distal metaphysis of the femur (Case 4).

Figure 2 Twelve-year-old female with giant cell rich osteosarcoma in the metaphysis of the distal radius (Case 2). (A) Initial radiograph shows a purely osteolytic lesion with cortical destruction. (B) During diagnostic delay of 2 months, the lesion showed marked progression.

Figure 3 Twenty-one-year-old male showing a huge scapula mass (Case 9). (A) Plain radiograph shows a purely osteolytic lesion in the scapula with a huge soft tissue shadow. (B) T1-weighted post-enhancement axial magnetic resonance imaging shows destruction of the scapula and marked extra-osseous mass formation.
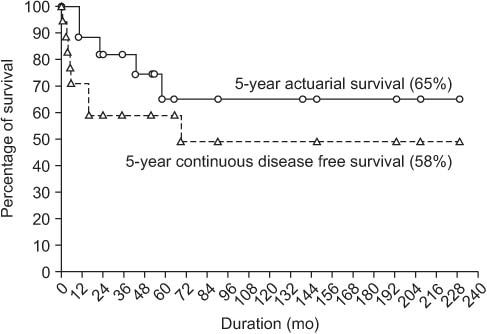
Figure 4 Five-year continuous disease free and actuarial survival of 17 patients with giant-cell rich osteosarcoma.

Figure 5 Continuous disease free survival of patients with adequate and inadequate diagnosis (p=0.14).
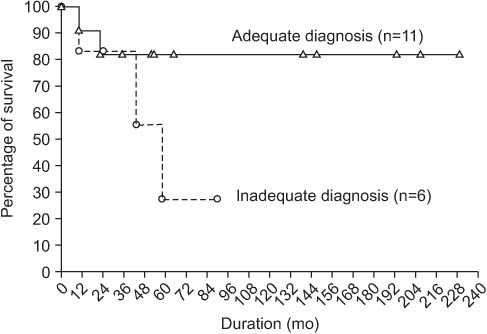
Figure 6 Actuarial survival of patients with adequate and inadequate diagnosis (p=0.14).
Reference
-
1. Moore DD, Luu HH. Osteosarcoma. Cancer Treat Res. 2014; 162:65–92.
Article2. Messerschmitt PJ, Garcia RM, Abdul-Karim FW, Greenfield EM, Getty PJ. Osteosarcoma. J Am Acad Orthop Surg. 2009; 17:515–527.
Article3. Bathurst N, Sanerkin N, Watt I. Osteoclast-rich osteosarcoma. Br J Radiol. 1986; 59:667–673.
Article4. Wang CS, Yin QH, Liao JS, Lou JH, Ding XY, Zhu YB. Giant cell-rich osteosarcoma in long bones: clinical, radiological and pathological features. Radiol Med. 2013; 118:1324–1334.
Article5. Shinozaki T, Fukuda T, Watanabe H, Takagishi K. Giant cell-rich osteosarcoma simulating giant cell tumor of bone. Kita Kanto Igaku. 2004; 54:147–151.
Article6. Brouns F, Stas M, De Wever I. Delay in diagnosis of soft tissue sarcomas. Eur J Surg Oncol. 2003; 29:440–445.
Article7. Sato K, Yamamura S, Iwata H, Sugiura H, Nakashima N, Nagasaka T. Giant cell-rich osteosarcoma: a case report. Nagoya J Med Sci. 1996; 59:151–157.8. Mirra JM. Bone tumors: clinical, radiologic and pathologic correlation. Philadelphia: Lea and Febiger;1989. p. 326–333.9. Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980; 153:106–120.
Article10. Gambarotti M, Donato M, Alberghini M, Vanel D. A strange giant cell tumor. Eur J Radiol. 2011; 77:3–5.
Article11. Huang J, Jiang Z, Zhang H. Clinicopathologic differential diagnosis of giant cell-rich osteosarcoma and giant cell tumor of bone. Zhonghua Bing Li Xue Za Zhi. 2014; 43:379–382.12. Takeuchi A, Lewis VO, Satcher RL, Moon BS, Lin PP. What are the factors that affect survival and relapse after local recurrence of osteosarcoma? Clin Orthop Relat Res. 2014; 472:3188–3195.
Article13. Ferrari S, Bertoni F, Mercuri M, et al. Predictive factors of disease-free survival for non-metastatic osteosarcoma of the extremity: an analysis of 300 patients treated at the Rizzoli Institute. Ann Oncol. 2001; 12:1145–1150.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Giant Cell Tumor with an Unusual Cartilage Matrix: A Case Report
- Denosumab-Treated Giant Cell Tumor of the Bone Mimicking Low-Grade Central Osteosarcoma
- Malignant Transformation of Benign Giant Cell Tumor
- Osteocalcin expression in primary bone tumors: in situ hybridization and immunohistochemical study
- Cutaneous Metastasis of Giant Cell-Rich Osteosarcoma
