Alveolar ridge augmentation with the perforated and nonperforated bone grafts
- Affiliations
-
- 1Department of Dental Materials and Prosthodontics, Araraquara School of Dentistry, UNESP Univ Estadual Paulista, Campus Araraquara, Araraquara, Brazil. erica.fobusp@yahoo.com.br
- 2Department of Diagnosis and Surgery, Araraquara School of Dentistry, UNESP Univ Estadual Paulista, Campus Araraquara, Araraquara, Brazil.
- 3Department of Morphology, Araraquara School of Dentistry, Sao Paulo State University, Araraquara, Brazil.
- KMID: 1845880
- DOI: http://doi.org/10.5051/jpis.2014.44.1.33
Abstract
- PURPOSE
Autogenous bones are frequently used because of their lack of antigenicity, but good osteoconductive and osteoinductive properties. This study evaluated the biological behavior of perforated and nonperforated cortical block bone grafts.
METHODS
Ten nonsmoking patients who required treatment due to severe resorption of the alveolar process and subsequent implant installation were included in the study. The inclusion criteria was loss of one or more teeth; the presence of atrophy of the alveolar process with the indication of reconstruction procedures to allow rehabilitation with dental implants; and the absence of systemic disease, local infection, or inflammation. The patients were randomly divided into two groups based on whether they received a perforated (inner surface) or nonperforated graft. After a 6-month healing period, a biopsy was performed and osseointegrated implants were installed in the same procedure.
RESULTS
Fibrous connective tissue was evident at the interface in patients who received nonperforated grafts. However, full union between the graft and host bed was visible in those who had received a perforated graft.
CONCLUSIONS
We found that cortical inner side perforations at donor sites increased the surface area and opened the medullary cavity. Our results indicate an increased rate of graft incorporation in patients who received such perforated grafts.
Keyword
MeSH Terms
Figure
-
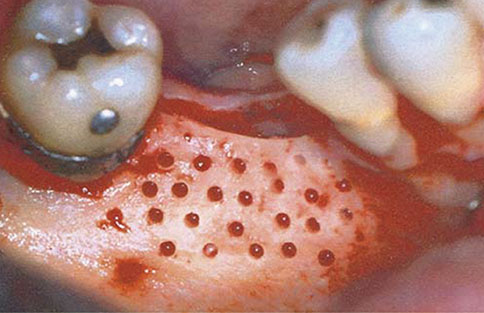
Figure 1 Receptor site before reconstruction.

Figure 2 Perforation of the graft's inner surface.

Figure 3 Nonperforated grafts fixed to the host bed.
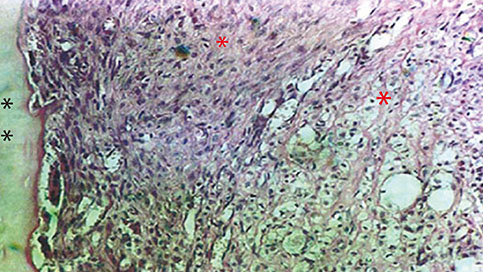
Figure 4 On the inner side of the nonperforated bone graft, observations of immature bone, large trabecular spaces, and some areas of newly formed bone is possible (H&E, ×250). Black asterisks indicate the inner side of nonperforated bone graft and the presence of osteoclasts and bone resorption characterized by the presence of innumerous inflammatory cells like macrophages. Red asterisks indicate recently formed connective tissue with innumerous blood vessels.
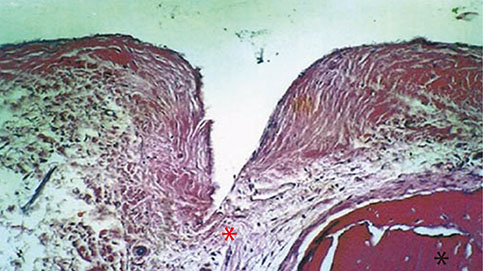
Figure 5 Nonperforated bone graft interface and the host bed with immature tissue (H&E, ×250). Black asterisk indicates the nonperforated bone graft with osteoclasts present. Red asterisk indicates the immature connective tissue interface in the supracrestal region.
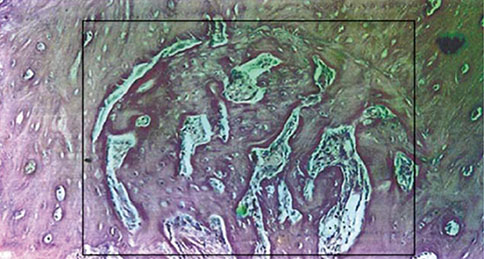
Figure 6 The inner side of the perforated bone graft with the perforated region created by cylindrical burs. Neoformed bone tissue characterized by the presence of innumerous osteocytes and medullary space and remodeling bone tissue with various osteoclasts are also present (H&E, ×250).
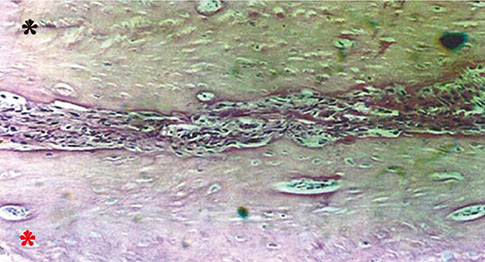
Figure 7 Perforated region of the bone graft and host bed with a slight presence of connective tissue (H&E, ×250). Black asterisk indicates bone tissue from the receptor bed with innumerous osteocytes. Red asterisk indicates the inner side of the perforated bone tissue with meduallary spaces, osteoclasts, and osteocytes.
Cited by 1 articles
-
Alveolar ridge preservation with a collagen material: a randomized controlled trial
Sigmar Schnutenhaus, Isabel Doering, Jens Dreyhaupt, Heike Rudolph, Ralph G. Luthardt
J Periodontal Implant Sci. 2018;48(4):236-250. doi: 10.5051/jpis.2018.48.4.236.
Reference
-
1. Oikarinen KS, Sandor GK, Kainulainen VT, Salonen-Kemppi M. Augmentation of the narrow traumatized anterior alveolar ridge to facilitate dental implant placement. Dent Traumatol. 2003; 19:19–29.
Article2. Chiapasco M, Zaniboni M, Rimondini L. Autogenous onlay bone grafts vs. alveolar distraction osteogenesis for the correction of vertically deficient edentulous ridges: a 2-4-year prospective study on humans. Clin Oral Implants Res. 2007; 18:432–440.
Article3. Jensen J, Sindet-Pedersen S. Autogenous mandibular bone grafts and osseointegrated implants for reconstruction of the severely atrophied maxilla: a preliminary report. J Oral Maxillofac Surg. 1991; 49:1277–1287.
Article4. Garg AK, Morales MJ, Navarro I, Duarte F. Autogenous mandibular bone grafts in the treatment of the resorbed maxillary anterior alveolar ridge: rationale and approach. Implant Dent. 1998; 7:169–176.
Article5. Schwartz-Arad D, Levin L. Intraoral autogenous block onlay bone grafting for extensive reconstruction of atrophic maxillary alveolar ridges. J Periodontol. 2005; 76:636–641.
Article6. Misch CM, Misch CE, Resnik RR, Ismail YH. Reconstruction of maxillary alveolar defects with mandibular symphysis grafts for dental implants: a preliminary procedural report. Int J Oral Maxillofac Implants. 1992; 7:360–366.7. Scaf de Molon R, de Avila ED, Scartezini GR, Bonini Campos JA, Vaz LG, Real Gabrielli MF, et al. In vitro comparison of 1.5 mm vs. 2.0 mm screws for fixation in the sagittal split osteotomy. J Craniomaxillofac Surg. 2011; 39:574–577.
Article8. Buser D, Dula K, Belser UC, Hirt HP, Berthold H. Localized ridge augmentation using guided bone regeneration. II. Surgical procedure in the mandible. Int J Periodontics Restorative Dent. 1995; 15:10–29.9. Sjöström M, Lundgren S, Sennerby L. A histomorphometric comparison of the bone graft-titanium interface between interpositional and onlay/inlay bone grafting techniques. Int J Oral Maxillofac Implants. 2006; 21:52–62.10. Lundgren S, Rasmusson L, Sjostrom M, Sennerby L. Simultaneous or delayed placement of titanium implants in free autogenous iliac bone grafts. Histological analysis of the bone graft-titanium interface in 10 consecutive patients. Int J Oral Maxillofac Surg. 1999; 28:31–37.
Article11. Lew D, Marino AA, Startzell JM, Keller JC. A comparative study of osseointegration of titanium implants in corticocancellous block and corticocancellous chip grafts in canine ilium. J Oral Maxillofac Surg. 1994; 52:952–958.
Article12. Faria PE, Okamoto R, Bonilha-Neto RM, Xavier SP, Santos AC, Salata LA. Immunohistochemical, tomographic and histological study on onlay iliac grafts remodeling. Clin Oral Implants Res. 2008; 19:393–401.
Article13. Rompen EH, Biewer R, Vanheusden A, Zahedi S, Nusgens B. The influence of cortical perforations and of space filling with peripheral blood on the kinetics of guided bone generation. A comparative histometric study in the rat. Clin Oral Implants Res. 1999; 10:85–94.
Article14. Delloye C, Simon P, Nyssen-Behets C, Banse X, Bresler F, Schmitt D. Perforations of cortical bone allografts improve their incorporation. Clin Orthop Relat Res. 2002; (396):240–247.
Article15. Smolka W, Eggensperger N, Carollo V, Ozdoba C, Iizuka T. Changes in the volume and density of calvarial split bone grafts after alveolar ridge augmentation. Clin Oral Implants Res. 2006; 17:149–155.
Article16. Pallesen L, Schou S, Aaboe M, Hjorting-Hansen E, Nattestad A, Melsen F. Influence of particle size of autogenous bone grafts on the early stages of bone regeneration: a histologic and stereologic study in rabbit calvarium. Int J Oral Maxillofac Implants. 2002; 17:498–506.17. Sbordone L, Toti P, Menchini-Fabris GB, Sbordone C, Piombino P, Guidetti F. Volume changes of autogenous bone grafts after alveolar ridge augmentation of atrophic maxillae and mandibles. Int J Oral Maxillofac Surg. 2009; 38:1059–1065.
Article18. Acocella A, Bertolai R, Colafranceschi M, Sacco R. Clinical, histological and histomorphometric evaluation of the healing of mandibular ramus bone block grafts for alveolar ridge augmentation before implant placement. J Craniomaxillofac Surg. 2010; 38:222–230.
Article19. Slotte C, Lundgren D. Impact of cortical perforations of contiguous donor bone in a guided bone augmentation procedure: an experimental study in the rabbit skull. Clin Implant Dent Relat Res. 2002; 4:1–10.
Article20. Barbosa DZ, de Assis WF, Shirato FB, Moura CC, Silva CJ, Dechichi P. Autogenous bone graft with or without perforation of the receptor bed: histologic study in rabbit calvaria. Int J Oral Maxillofac Implants. 2009; 24:463–468.21. Kostopoulos L, Karring T. Augmentation of the rat mandible using guided tissue regeneration. Clin Oral Implants Res. 1994; 5:75–82.
Article22. Nishimura I, Shimizu Y, Ooya K. Effects of cortical bone perforation on experimental guided bone regeneration. Clin Oral Implants Res. 2004; 15:293–300.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The study on the bone resorption rate after vertical alveolar ridge augmentation
- Ridge augmentation using of hard tissue replacement(htrtm): a case report
- Ridge Augmentation Using Block Type of Autogenous Tooth Bone Graft Material in Severe Alveolar Bone Resorption of Single Tooth: Case Report
- Clinical usages of ramal autogenous bone grafts in dental implant surgery
- Implant Placement Using Alveolar Ridge Split in Atrophic Maxillary Alveolar Bone
