Diagnosis of Benign and Metastatic Bone Lesions on Breast MRI in Patients with Breast Cancer
- Affiliations
-
- 1Department of Radiology, Ewha Womans University Mokdong Hospital, Ewha Womans University School of Medicine, Seoul, Korea. escha@ewha.ac.kr
- KMID: 1839423
- DOI: http://doi.org/10.3348/jksr.2014.70.2.137
Abstract
- PURPOSE
To differentiate between the MRI findings for benign bone lesion and metastasis detected by breast MRI in patients with breast cancer and to evaluate the conspicuity of bone lesions according to MR sequences.
MATERIALS AND METHODS
In 14 patients with 15 bone lesions, the MRI findings were statistically analyzed to differentiate between benign bone lesion and metastasis. We considered margin, signal intensity on T2-weighted image (T2WI) with spectral attenuated inversion recovery (SPAIR), enhancement, and patterns of bone lesions (focal mass, diffuse infiltration, and extraosseous soft tissue change), as well as the conspicuity of bone lesions in each MR sequence.
RESULTS
There was a statistically significant difference in the frequency of a solitary focal mass pattern between benign bone lesion and metastasis (p = 0.044). The margin, signal intensity on T2WI with SPAIR, and enhancement were not significantly different between benign bone lesion and metastasis. Both T2WI with SPAIR and delayed phase of contrast enhanced MRI were superior to other sequences in terms of lesion conspicuity.
CONCLUSION
A solitary focal mass pattern indicates a high probability of benign bone lesion on breast MRI in patients with breast cancer. Bone lesions tend to have greater conspicuity on T2WI with SPAIR and delayed phase image of contrast enhanced MRI, compared to results for other MR sequences.
Figure
-

Fig. 1 Illustration of pattern of bone lesions in breast MRI. Focal mass pattern represents a round or oval mass confined in marrow space (A) or an expansile mass (B). Diffuse infiltration pattern represents signal intensity change of whole marrow space (C) or part of marrow space (D), which are confined in marrow space without cortical destruction. Extraosseous soft tissue change pattern represents extraosseous mass (E) or signal intensity change of periosteal soft tissue (F).
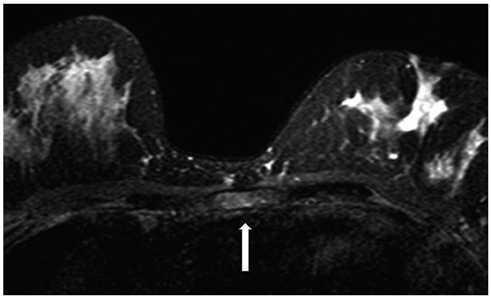
Fig. 2 A 47-year-old female with sternal metastasis showing diffuse infiltration pattern. Bone lesion with diffuse infiltration (arrow) is noted in sternum on axial T2-weighted image with spectral attenuated inversion recovery.
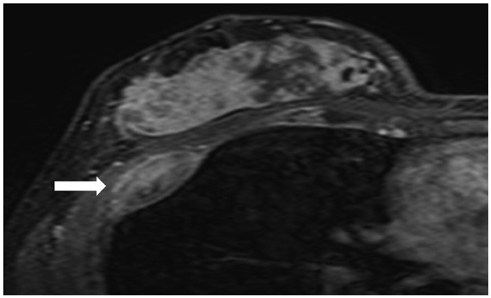
Fig. 3 A 31-year-old female with rib metastasis showing extraosseous soft tissue change pattern. Extraosseous mass formation (arrow) is noted in right lower rib on dynamic enhanced MRI (delay phase).
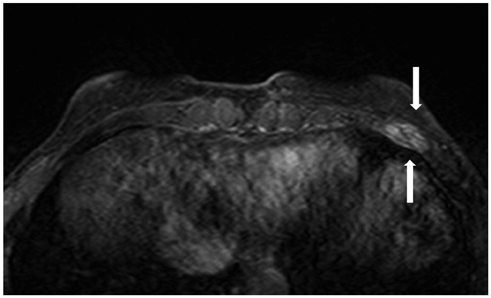
Fig. 4 A 50-year-old female with fracture showing extraosseous soft tissue change pattern. Fracture line and surrounding bone marrow edema (arrows) is noted in left lower rib on axial T2-weighted image with spectral attenuated inversion recovery.

Fig. 5 A 43-year-old female with fibrous dysplasia showing focal mass pattern. A. Dynamic enhanced MR image (delay phase) shows a well defined expansile bone lesion (arrow) in left 3rd rib. B. Radiography (rib series) shows well defined osteolytic bone lesion (arrow) at left 3rd rib anterior arc, representing typical feature of fibrous dysplasia.
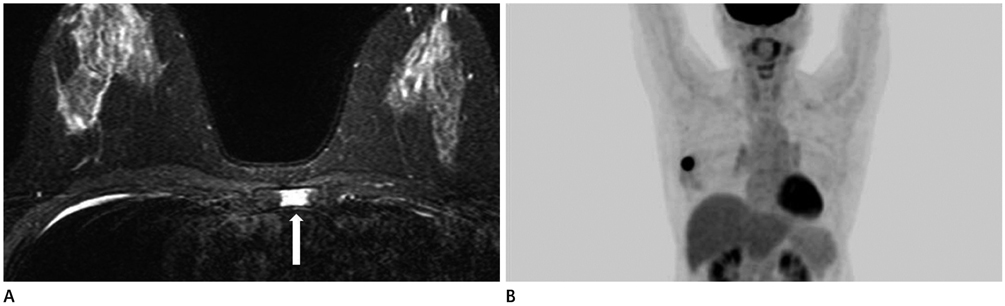
Fig. 6 A 60-year-old female with bone lesion showing diffuse infiltration pattern in sternum. A. On initial breast T2 weighted MRI with spectral attenuated inversion recovery, there are segmental infiltration (arrow) in left side sternum, which is possibility of sternal metastasis. However, this sternum lesion is not changed on follow-up MRI, 5 months later (not shown). B. Positron emission tomography-CT shows no definite uptake in sternal area. This bone lesion has been considered as probable benign bone lesion. This patient has been free of cancer recurrence for 3 years since she had been diagnosed breast cancer.
Reference
-
1. Korean Breast Cancer Society. 2013 Breast cancer facts and figures. Seoul: Korean Breast Cancer Society;2013. 1:p. 4–13.2. Orel SG, Schnall MD. MR imaging of the breast for the detection, diagnosis, and staging of breast cancer. Radiology. 2001; 220:13–30.3. Schnall MD, Blume J, Bluemke DA, DeAngelis GA, DeBruhl N, Harms S, et al. Diagnostic architectural and dynamic features at breast MR imaging: multicenter study. Radiology. 2006; 238:42–53.4. Yabuuchi H, Kuroiwa T, Kusumoto C, Fukuya T, Ohno S, Hachitanda Y. Incidentally detected lesions on contrast-enhanced MR imaging in candidates for breast-conserving therapy: correlation between MR findings and histological diagnosis. J Magn Reson Imaging. 2006; 23:486–492.5. Yabuuchi H, Matsuo Y, Okafuji T, Kamitani T, Soeda H, Setoguchi T, et al. Enhanced mass on contrast-enhanced breast MR imaging: lesion characterization using combination of dynamic contrast-enhanced and diffusion-weighted MR images. J Magn Reson Imaging. 2008; 28:1157–1165.6. Rausch DR. Spectrum of extra-mammary findings on breast MRI: a pictorial review. Breast J. 2008; 14:592–594.7. Rinaldi P, Costantini M, Belli P, Giuliani M, Bufi E, Fubelli R, et al. Extra-mammary findings in breast MRI. Eur Radiol. 2011; 21:2268–2276.8. Greene FL, Page DL, Fleming ID, Fritz A, Balch CM, Haller DG, et al. American Joint Committee on Cancer. AJCC Cancer Staging Manual. 6th ed. New York: Springer-Verlag;2002.9. Liu T, Cheng T, Xu W, Yan WL, Liu J, Yang HL. A meta-analysis of 18FDG-PET, MRI and bone scintigraphy for diagnosis of bone metastases in patients with breast cancer. Skeletal Radiol. 2011; 40:523–531.10. Li S, Sun F, Jin ZY, Xue HD, Li ML. Whole-body diffusion-weighted imaging: technical improvement and preliminary results. J Magn Reson Imaging. 2007; 26:1139–1144.11. Hu S, Lustig M, Chen AP, Crane J, Kerr A, Kelley DA, et al. Compressed sensing for resolution enhancement of hyperpolarized 13C flyback 3D-MRSI. J Magn Reson. 2008; 192:258–264.12. Grankvist J, Fisker R, Iyer V, Fründ ET, Simonsen C, Christensen T, et al. MRI and PET/CT of patients with bone metastases from breast carcinoma. Eur J Radiol. 2012; 81:e13–e18.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Magnetic Resonance Findings of Breast Diseases
- Clinical Outcome of Magnetic Resonance Imaging-Detected Additional Lesions in Breast Cancer Patients
- Clinical Applications of Breast MRI
- Application of Biomarkers for the Prediction and Diagnosis of Bone Metastasis in Breast Cancer
- Incidental Extramammary Findings on Preoperative Breast MRI in Breast Cancer Patients: A Pictorial Essay
