J Korean Surg Soc.
2012 Apr;82(4):227-231. 10.4174/jkss.2012.82.4.227.
Postoperative pneumoperitoneum: guilty or not guilty?
- Affiliations
-
- 1Department of Surgery, Chonbuk National University Medical School, Jeonju, Korea. gsminro@chonbuk.ac.kr
- KMID: 1820070
- DOI: http://doi.org/10.4174/jkss.2012.82.4.227
Abstract
- PURPOSE
The aim of this study was to determine the incidence and duration of postoperative pneumoperitoneum on plain radiographs and to identify the radiologic findings associated with anastomotic leakage.
METHODS
A retrospective analysis was conducted on plain radiographs of 384 patients who underwent intra-abdominal anastomoses between March 2005 and December 2008.
RESULTS
Of the 384 patients, 93 patients (24.2%) had postoperative pneumoperitoneums. Of the 93 patients, 86 patients (92.5%) had physiologic pneumoperitoneums and 7 patients (7.5%) had pneumoperitoneums associated with anastomotic leakage. The initial air height was significantly greater in the leakage group than the physiologic air group (12.16 +/- 7.65 mm vs. 7.71 +/- 5.08 mm, P = 0.04). The area under the receiver operating characteristic curve of the initial height of free air for anastomotic leakage was 0.69 (95% confidence interval, 0.59 to 0.78). The best cut-off point was 11.7 mm. The height of the pneumoperitoneum increased with time in the leakage group. Ileus was significantly more prevalent in the leakage group than the physiologic air group (P < 0.01).
CONCLUSION
Postoperative pneumoperitoneum is a common phenomenon after abdominal surgery. An initial air height >11.7 mm, increasing air height over time, and the presence of ileus on plain radiographs suggest a high likelihood of anastomotic leakage.
Figure
-
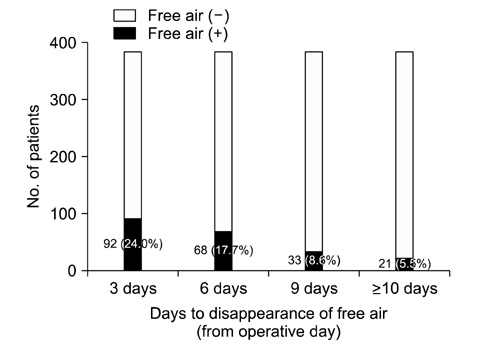
Fig. 1 Prevalence of free air (n = 384) with time.

Fig. 2 The receiver operating characteristic (ROC) curve of initial height of free air in patients with anastomotic leakage.
Reference
-
1. Han KS, Kong SK, Pyo CH. Pneumoperitoneum in acute diffuse peritonitis due to perforation of gastro-intestinal tract. J Korean Surg Soc. 1970. 12:55–58.2. Bevan PG. Incidence of post-operative pneumoperitoneum and its significance. Br Med J. 1961. 2:605–609.3. Bryant LR, Wiot JF, Kloecker RJ. A study of the factors affecting the incidence and duration of postoperative pneumoperitoneum. Surg Gynecol Obstet. 1963. 117:145–150.4. Harrison I, Litwer H, Gerwig WH Jr. Studies on the incidence and duration of postoperative pneumoperitoneum. Ann Surg. 1957. 145:591–594.5. Stapakis JC, Thickman D. Diagnosis of pneumoperitoneum: abdominal CT vs. upright chest film. J Comput Assist Tomogr. 1992. 16:713–716.6. Mansy HA, Royston TJ, Sandler RH. Use of abdominal percussion for pneumoperitoneum detection. Med Biol Eng Comput. 2002. 40:439–446.7. Earls JP, Dachman AH, Colon E, Garrett MG, Molloy M. Prevalence and duration of postoperative pneumoperitoneum: sensitivity of CT vs left lateral decubitus radiography. AJR Am J Roentgenol. 1993. 161:781–785.8. Markowitz SK, Ziter FM Jr. The lateral chest film and pneumoperitoneum. Ann Emerg Med. 1986. 15:425–427.9. Miller RE, Nelson SW. The roentgenologic demonstration of tiny amounts of free intraperitoneal gas: experimental and clinical studies. Am J Roentgenol Radium Ther Nucl Med. 1971. 112:574–585.10. Tang CL, Yeong KY, Nyam DC, Eu KW, Ho YH, Leong AF, et al. Postoperative intra-abdominal free gas after open colorectal resection. Dis Colon Rectum. 2000. 43:1116–1120.11. Gayer G, Jonas T, Apter S, Amitai M, Shabtai M, Hertz M. Postoperative pneumoperitoneum as detected by CT: prevalence, duration, and relevant factors affecting its possible significance. Abdom Imaging. 2000. 25:301–305.12. Schauer PR, Page CP, Ghiatas AA, Miller JE, Schwesinger WH, Sirinek KR. Incidence and significance of subdiaphragmatic air following laparoscopic cholecystectomy. Am Surg. 1997. 63:132–136.13. Wiot JF, Benton C, McAlister WH. Postoperative pneumoperitoneum in children. Radiology. 1967. 89:285–288.14. Rice RP, Thompson WM, Gedgaudas RK. The diagnosis and significance of extraluminal gas in the abdomen. Radiol Clin North Am. 1982. 20:819–837.15. Millitz K, Moote DJ, Sparrow RK, Girotti MJ, Holliday RL, McLarty TD. Pneumoperitoneum after laparoscopic cholecystectomy: frequency and duration as seen on upright chest radiographs. AJR Am J Roentgenol. 1994. 163:837–839.16. Gayer G, Hertz M, Zissin R. Postoperative pneumoperitoneum: prevalence, duration, and possible significance. Semin Ultrasound CT MR. 2004. 25:286–289.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Preliminary Research for Making Judgment on Not Guilty by Reason of Insanity and Guilty but Mentally Ill
- Guilty, or not guilty?: a short story of propofol abuse
- Comparing postoperative pain in various pressure pneumoperitoneum of laparoscopic cholecystectomy: a double-blind randomized controlled study
- Family Burden of Schizophrenics in the Primary Caregivers and Siblings
- Pneumoperitoneum due to Emphysematous Cholecystitis
