J Cardiovasc Ultrasound.
2015 Jun;23(2):100-102. 10.4250/jcu.2015.23.2.100.
A Hypereosinophilic Syndrome with Cardiac Involvement from Thrombotic Stage to Fibrotic Stage
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea. scchae@knu.ac.kr
- KMID: 1806918
- DOI: http://doi.org/10.4250/jcu.2015.23.2.100
Abstract
- Cardiac involvement is a major cause of morbidity and mortality in hypereosinophilic syndrome (HES). It is classified into 3 stages by the degree of eosinophils-mediated heart injury; acute necrotic stage, thrombotic stage, and fibrotic stage. Nonetheless, definitive evidence that each patient passes sequentially through these stages is lacking. We present a case of 48-year-old male patient with dyspnea and peripheral edema who underwent valve replacement surgery due to severe mitral regurgitation. After the valve replacement, HES with cardiac involvement in the thrombotic stage was diagnosed. In the follow-up study, the patient progressed into fibrotic stage of HES.
MeSH Terms
Figure
-
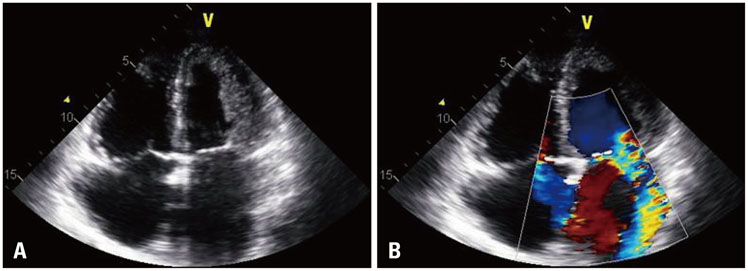
Fig. 1 Preoperative echocardiography shows mild endocardial thickening in lateral wall and apex of left ventricle (A) with severe mitral regurgitation and moderate tricuspid regurgitation (B).

Fig. 2 Histopathologic analysis of left ventricle shows fibrin clot with blood clot, inflammatory cells (A) and eosinophil infiltration (B) (hematoxylin and eosin stain, × 200).
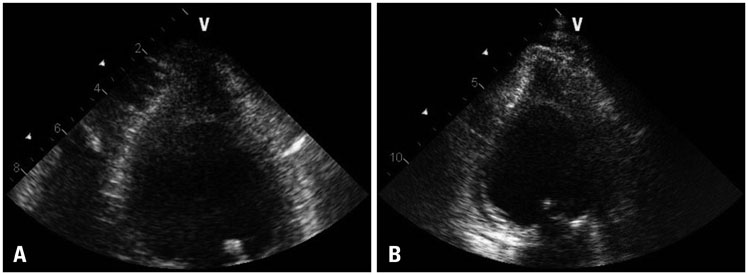
Fig. 3 Transthoracic echocardiographic study at 2 years after the operation shows an obliteration of left ventricular apex with homogenous echo density in apical 4 chamber (A) and 2 chamber (B) views.
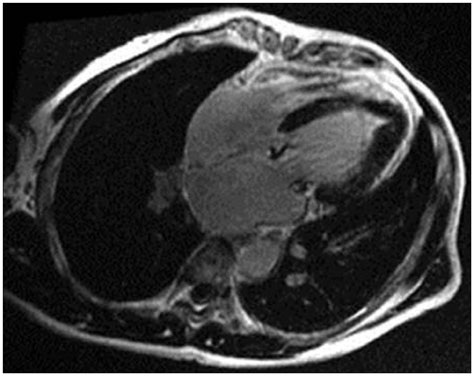
Fig. 4 Cardiac magnetic resonance imaging shows subendocardial delayed enhancement at apex.
Reference
-
1. Chusid MJ, Dale DC, West BC, Wolff SM. The hypereosinophilic syndrome: analysis of fourteen cases with review of the literature. Medicine (Baltimore). 1975; 54:1–27.2. Ogbogu PU, Bochner BS, Butterfield JH, Gleich GJ, Huss-Marp J, Kahn JE, Leiferman KM, Nutman TB, Pfab F, Ring J, Rothenberg ME, Roufosse F, Sajous MH, Sheikh J, Simon D, Simon HU, Stein ML, Wardlaw A, Weller PF, Klion AD. Hypereosinophilic syndrome: a multicenter, retrospective analysis of clinical characteristics and response to therapy. J Allergy Clin Immunol. 2009; 124:1319–1325.e3.
Article3. Ogbogu PU, Rosing DR, Horne MK 3rd. Cardiovascular manifestations of hypereosinophilic syndromes. Immunol Allergy Clin North Am. 2007; 27:457–475.
Article4. Weller PF, Bubley GJ. The idiopathic hypereosinophilic syndrome. Blood. 1994; 83:2759–2779.
Article5. Parrillo JE, Borer JS, Henry WL, Wolff SM, Fauci AS. The cardiovascular manifestations of the hypereosinophilic syndrome. Prospective study of 26 patients, with review of the literature. Am J Med. 1979; 67:572–582.6. Sen T, Gungor O, Akpinar I, Cetin M, Tufekcioglu O, Golbasi Z. Cardiac involvement in hypereosinophilic syndrome. Tex Heart Inst J. 2009; 36:628–629.7. Zientek DM, King DL, Dewan SJ, Harford PH, Youman DJ, Hines TR. Hypereosinophilic syndrome with rapid progression of cardiac involvement and early echocardiographic abnormalities. Am Heart J. 1995; 130:1295–1298.
Article8. Madhwal S, Goldberg J, Barcena J, Guha A, Gogate P, Cmolik B, Elgudin Y. Unusual cause of acute mitral regurgitation: idiopathic hypereosinophilic syndrome. Ann Thorac Surg. 2012; 93:974–977.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Hypereosinophilic Syndrome Presenting as Pericardial Effusion, Myocarditis and Ascites
- A case of idiopathic hypereosinophilic syndrome manifested as regional wall motion abnormalities in echocardiogram and pericardial effusion
- A case of idiopathic hypereosinophilic syndrome presenting multiple organ injuries with eyeball involvement
- Pulmonary Involvement of Hypereosinophilic Syndrome: High-Resolution CT Findings in Three Patients
- A Case of Huge Left Ventricular Thrombus Associated with Hypereosinophilic Syndrome
