A Case of Hypereosinophilic Syndrome Presenting as Pericardial Effusion, Myocarditis and Ascites
- Affiliations
-
- 1Department of Internal Medicine, Soonchunghyang University Cheonan Hospital, Cheonan, Korea. matsalong@schch.co.kr
- KMID: 2225765
- DOI: http://doi.org/10.4070/kcj.2008.38.8.436
Abstract
- Hypereosinophilic syndrome is a clinical disorder characterized by peripheral eosinophilia and eosinophilic infiltration of multiple organ systems, including the cardiovascular system. The manifestations are variable, but cardiac involvement is the major source of morbidity and mortality, and several case reports have highlighted the various types of cardiac involvement. However, no reported case has simultaneously presented with pericardial effusion, myocarditis, and ascites. We report a case of a 28-year-old woman with hypereosinophilic syndrome involving both the heart and intra-abdominopelvic cavity.
Keyword
MeSH Terms
Figure
-

Fig. 1 Initial images. A: chest X-ray demonstrated cardiomegaly and bilateral pleural effusions. B: chest CT demonstrated pericardial effusion and bilateral pleural effusions. C: abdominal CT demonstrated ascites in the gallbladder fossa. D: pelvic CT demonstrated ascites in the pelvic cavity.
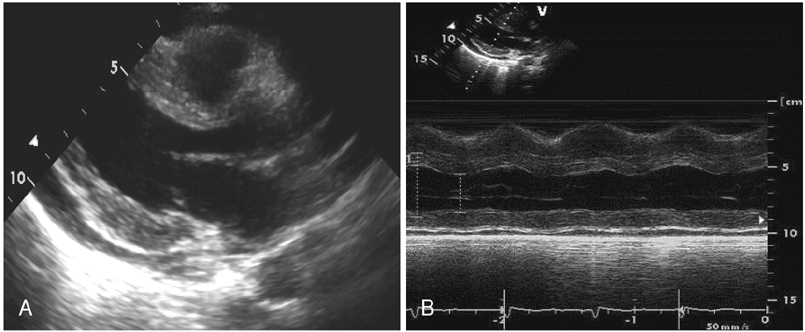
Fig. 2 Echocardiographic findings. A: 2D echocardiography (parasternal long axis view) demonstrated multiple regional wall motion abnormalities incompatible with the coronary territory, a moderate pericardial effusion of no hemodynamic significance, and increased thickening of the basal inferoposterior wall. B: M-mode echocardiography demonstrated a regional wall motion abnormality of the basal inferoposterior wall. There was mild left ventricular dysfunction (ejection fraction-45%), but no systolic wall thickening.

Fig. 3 Endomyocardial biopsy revealed a markedly increased number of eosinophils infiltrating the endomyocardial tissue. A: H & E stain, ×100. B: H & E stain, ×400. H & E: hematoxylin and eosin.

Fig. 4 Follow-up images. A: chest X-ray showed no cardiomegaly or pleural effusion. B: echocardiography showed that the pericardial effusion and abnormal echogenicity of the posterolateral wall had resolved. C, D: abdominal CT demonstrated marked improvement of ascites in the gallbladder fossa and pelvic cavity.
Reference
-
1. Weller PF, Bubley GJ. The idiopathic hypereosinophilic syndrome. Blood. 1994. 83:2759–2779.2. Chusid MJ, Dale DC, West BC, Wolff SM. The hypereosinophilic syndrome: analysis of fourteen cases with review of literature. Medicine. 1975. 54:1–27.3. Schenkein DP, Wolff SM. Hoffman R, editor. Eosinophilia and the hypereosinophilic syndrome. Hematology: Basic Principles and Practice. 1995. 2nd ed. New York: Churchill Livingstone;784.4. Ommen SR, Seward JB, Tajik AJ. Clinical and echocardiographic features of hypereosinophilic syndromes. Am J Cardiol. 2000. 86:110–113.5. Lee M, Hodges WG, Huggins TL, Lee EL. Eosinophilic gastroenteritis. South Med J. 1996. 89:189–194.6. Yoo K, Lee JH, Lee MS, et al. Eosinophilic gastroenteritis involving entire gastrointestinal tract with eosinophilic ascites. Korean J Gastrointest Endosc. 2001. 22:159–163.7. Parrillo JE, Fauci AS, Wolff SM. Therapy of the hypereosinophilic syndrome. Ann Intern Med. 1978. 89:167–172.8. Shin MS, Ann YM, Cho HK, Shin GJ, Jung NS, Cho SH. A case of eosinophilic myocarditis with hypereosionphilia showing myocardial edema. Korean Circ J. 1998. 28:296–303.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Idiopathic Hypereosinophilic Syndrome Manifested by Massive Pericardial Effusion
- Eosinophilic Endomyocarditis Combined With Pericardial and Pleural Effusion
- A case of idiopathic hypereosinophilic syndrome manifested as regional wall motion abnormalities in echocardiogram and pericardial effusion
- A case of primary hypothyroidism presenting with massive pericardial effusion and ascites
- Two Cases of Primary HypoThyroidism Presenting with Pericardial Effusion
