Endoscopic Assessment of Colorectal Cancer with Superficial or Deep Submucosal Invasion Using Magnifying Colonoscopy
- Affiliations
-
- 1Department of Endoscopy, Hiroshima University Hospital, Hiroshima, Japan. colon@hiroshima-u.ac.jp
- 2Department of Gastroenterology and Metabolism, Hiroshima University Hospital, Hiroshima, Japan.
- KMID: 1805295
- DOI: http://doi.org/10.5946/ce.2013.46.2.138
Abstract
- Among early colorectal carcinoma, endoscopic treatment is generally indicative for cases with intramucosal to submucosal (SM) superficial invasion, because cases with SM deep invasion should be treated surgically due to the risk of lymph node metastasis. It is important, therefore, to distinguish between superficial and deep SM invasion in early colorectal carcinoma prior to treatment. In this review we assessed the clinical usefulness and knack of pit pattern and narrow band imaging (NBI) diagnosis using magnifying observation. VN type pit pattern, type C3 in NBI Hiroshima classification and NBI type 3 in NBI international colorectal endoscopic (NICE) classification are useful predictors of SM deep invasion. In NBI magnifying observation evaluation of both the vascular pattern and surface pattern are important. We have to use pit pattern diagnosis and NBI magnifying diagnosis as the situation demands with the knowledge of both advantage and disadvantage in each diagnostic method.
Keyword
MeSH Terms
Figure
-
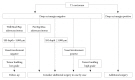
Fig. 1 Therapeutic strategy for colorectal submucosal (SM) carcinoma resected endoscopically (Japanese guideline for colorectal cancer treatment, 2010).

Fig. 2 Pit pattern classification of colorectal neoplasia (Adapted from Tanaka et al. Gastrointest Endosc 2006;64:604-613, with permission from Elsevier).

Fig. 3 Hakone agreement regarding the subclassification of type-V pit patterns (April 2004, Hakone). In April 2004, a consensus meeting was held in Hakone and the definitions of findings of type-V pit pattern-based diagnosis were unified. The type-V pit pattern was subclassified into type-VI, which represents an irregular glandular structure, and type-VN, which represents a clear amorphous region. The invasive pattern, highly irregular glands, and the scratch sign were included as indices for submucosal carcinomas. Of note, colorectal tumors with a clear amorphous region were defined as type-VN.

Fig. 4 (A) Irregular pit pattern (type-VI slightly irregular pit pattern). Magnifying observation images with crystal violet staining. These two lesions can be classified as the type-VI pit pattern with slight irregularity. No amorphous region is observed, but irregular pit structures such as different sizes and disordered arrangement (mainly, the structural atypia is irregular) are noted. (B) Irregular pit pattern (type-VI highly irregular pit pattern). Magnifying observation images with crystal violet staining. These two lesions can be classified as the type-VI pit pattern with high irregularity. No clear amorphous region is observed, but pit structures with an irregular, rough margin; a decrease in stainability in the stromal area (surface pattern); and an unclear pit margin (the pit opening is damaged or destroyed) are noted.

Fig. 5 A case of colorectal carcinoma with submucosal deep invasion. (A) Sessile polypoid lesion in standard colonoscopic view. (B) Indigo carmine dye spraying view. (C) Narrow band imaging magnifying view. Surface pattern is unclear to amorphous and there is an avascular area with scattered vessel (Hiroshima classification type C3). (D) Magnifying view with crystal violet staining. Center of the lesion shows amorphous (VN type pit pattern). (E) Cross section of surgically resected specimen shows deep subumucosal invasion with desmoplastic reaction (H&E stain, ×20).
Cited by 1 articles
-
Narrow Band Imaging as an Efficient and Economical Tool in Diagnosing Colorectal Polyps
Naoki Muguruma, Tetsuji Takayama
Clin Endosc. 2015;48(6):461-463. doi: 10.5946/ce.2015.48.6.461.
Reference
-
1. Tanaka S, Terasaki M, Hayashi N, Oka S, Chayama K. Warning for unprincipled colorectal endoscopic submucosal dissection: Accurate diagnosis and reasonable treatment strategy. Dig Endosc. 2013; 25:107–116. PMID: 23368854.
Article2. Watanabe T, Itabashi M, Shimada Y, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2010 for the treatment of colorectal cancer. Int J Clin Oncol. 2012; 17:1–29. PMID: 22002491.
Article3. Kunihiro M, Tanaka S, Haruma K, et al. Electrocautery snare resection stimulates cellular proliferation of residual colorectal tumor: an increasing gene expression related to tumor growth. Dis Colon Rectum. 2000; 43:1107–1115. PMID: 10950009.4. Kudo S, Tamura S, Nakajima T, Yamano H, Kusaka H, Watanabe H. Diagnosis of colorectal tumorous lesions by magnifying endoscopy. Gastrointest Endosc. 1996; 44:8–14. PMID: 8836710.
Article5. Tanaka S, Kaltenbach T, Chayama K, Soetikno R. High-magnification colonoscopy (with videos). Gastrointest Endosc. 2006; 64:604–613. PMID: 16996357.
Article6. Sakamoto T, Matsuda T, Matsumoto M, et al. Endoscopic features of poorly differentiated adnocarcinoma in the colorectm. Stomach Intest. 2010; 45:1750–1756.7. Kimura T, Yamamoto E, Yamano HO, et al. A novel pit pattern identifies the precursor of colorectal cancer derived from sessile serrated adenoma. Am J Gastroenterol. 2012; 107:460–469. PMID: 22233696.
Article8. Yao T, Sugai T, Iwashita A, et al. Histopathological characteristics and diagnostic criteria of SSA/P, from project research "potential of cancerization of colorectal serrated lesions" of the Japanese Society for Cancer of the Colon and Rectum. Stomach Intest. 2011; 46:442–448.9. Kanao H, Tanaka S, Oka S, et al. Clinical significance of type V(I) pit pattern subclassification in determining the depth of invasion of colorectal neoplasms. World J Gastroenterol. 2008; 14:211–217. PMID: 18186557.10. Masaki T, Katada C, Nakayama M, et al. Narrow band imaging in the diagnosis of intra-epithelial and invasive laryngeal squamous cell carcinoma: a preliminary report of two cases. Auris Nasus Larynx. 2009; 36:712–716. PMID: 19261406.
Article11. Gono K, Obi T, Yamaguchi M, et al. Appearance of enhanced tissue features in narrow-band endoscopic imaging. J Biomed Opt. 2004; 9:568–577. PMID: 15189095.
Article12. Sano Y, Muto M, Tajiri H, Ohtsu A, Yoshida S. Optical/digital chromoendoscopy during colonoscopy using narrow-band imaging system. Dig Endosc. 2005; 17(Suppl 1):S43–S48.
Article13. Oba S, Tanaka S, Oka S, et al. Characterization of colorectal tumors using narrow-band imaging magnification: combined diagnosis with both pit pattern and microvessel features. Scand J Gastroenterol. 2010; 45:1084–1092. PMID: 20350257.
Article14. Ikematsu H, Matsuda T, Emura F, et al. Efficacy of capillary pattern type IIIA/IIIB by magnifying narrow band imaging for estimating depth of invasion of early colorectal neoplasms. BMC Gastroenterol. 2010; 10:33. PMID: 20346170.
Article15. Kanao H, Tanaka S, Oka S, Hirata M, Yoshida S, Chayama K. Narrow-band imaging magnification predicts the histology and invasion depth of colorectal tumors. Gastrointest Endosc. 2009; 69(3 Pt 2):631–636. PMID: 19251003.
Article16. Wada Y, Kudo SE, Kashida H, et al. Diagnosis of colorectal lesions with the magnifying narrow-band imaging system. Gastrointest Endosc. 2009; 70:522–531. PMID: 19576581.
Article17. Tanaka S, Sano Y. Aim to unify the narrow band imaging (NBI) magnifying classification for colorectal tumors: current status in Japan from a summary of the consensus symposium in the 79th Annual Meeting of the Japan Gastroenterological Endoscopy Society. Dig Endosc. 2011; 23(Suppl 1):131–139. PMID: 21535219.
Article18. Hirata M, Tanaka S, Oka S, et al. Evaluation of microvessels in colorectal tumors by narrow band imaging magnification. Gastrointest Endosc. 2007; 66:945–952. PMID: 17963882.
Article19. Oba S, Tanaka S, Sano Y, Oka S, Chayama K. Current status of narrow-band imaging magnifying colonoscopy for colorectal neoplasia in Japan. Digestion. 2011; 83:167–172. PMID: 21266811.
Article20. Hewett DG, Kaltenbach T, Sano Y, et al. Validation of a simple classification system for endoscopic diagnosis of small colorectal polyps using narrow-band imaging. Gastroenterology. 2012; 143:599–607. PMID: 22609383.
Article21. Nakayama N, Tanaka S, Sano Y, et al. Validation of the narrow band imaging (NBI) international colorectal endoscopic (NICE) classification for prediction of deep submucosal invasive carcinoma. Gastrointest Endosc. 2012; 75:AB338–AB339.22. Takata S, Tanaka S, Hayashi N, et al. Characteristic magnifying narrow-band imaging features of colorectal tumors in each growth type. Int J Colorectal Dis. 2000; Epub 2012 Dec 4. DOI: http://dx.doi.org/10.1007/s00384-012-1612-6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Estimation of Invasion Depth: The First Key to Successful Colorectal ESD
- Endoscopic Diagnosis and Treatment of Colorectal Cancers
- Introduction: What Are New Roles of Current Colonoscopy?
- Polyp Detection, Characterization, and Management Using Narrow-Band Imaging with/without Magnification
- Diagnostic Accuracy and Interobserver Agreement in Predicting the Submucosal Invasion of Colorectal Tumors Using Gross Findings, Pit Patterns, and Microvasculatures
