Fenestration of liver cysts in polycystic liver disease to improve quality of life: a case report and literature review
- Affiliations
-
- 1Division of Hepatobiliary Surgery and Liver Transplantation, Departments of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. shwang@amc.seoul.kr
- KMID: 1802239
- DOI: http://doi.org/10.14701/kjhbps.2015.19.1.40
Abstract
- Polycystic liver disease (PCLD) is characterized by a large number of liver cysts scattered throughout the liver parenchyma. We herein intend to present the beneficial effect of palliative fenestration treatment on quality of life in a patient with symptomatic PCLD. A 48-year-old female patient had been followed up for 5 years for both polycystic liver and kidney diseases at another institution. During follow-up for last 1 year, we recognized that she had barely maintained her ability of function in daily activities due to progressive worsening of fatigue and dyspnea on exertion. The patient finally underwent surgical fenestration treatment. Multiple cysts in the enlarged liver were opened and the cyst walls were excised with electrocautery. No surgical complication occurred and the patient was discharged 10 days after the open fenestration surgery. The total liver volume was 3,870 ml before surgery and 3,125 ml at 1 week after surgery, showing a volume reduction of 19.3%. After surgery, her performance status improved significantly. In the present case, significant improvement in quality of life and daily activity performance was achieved after open fenestration treatment over 18 months of follow-up without disease recurrence.
MeSH Terms
Figure
-
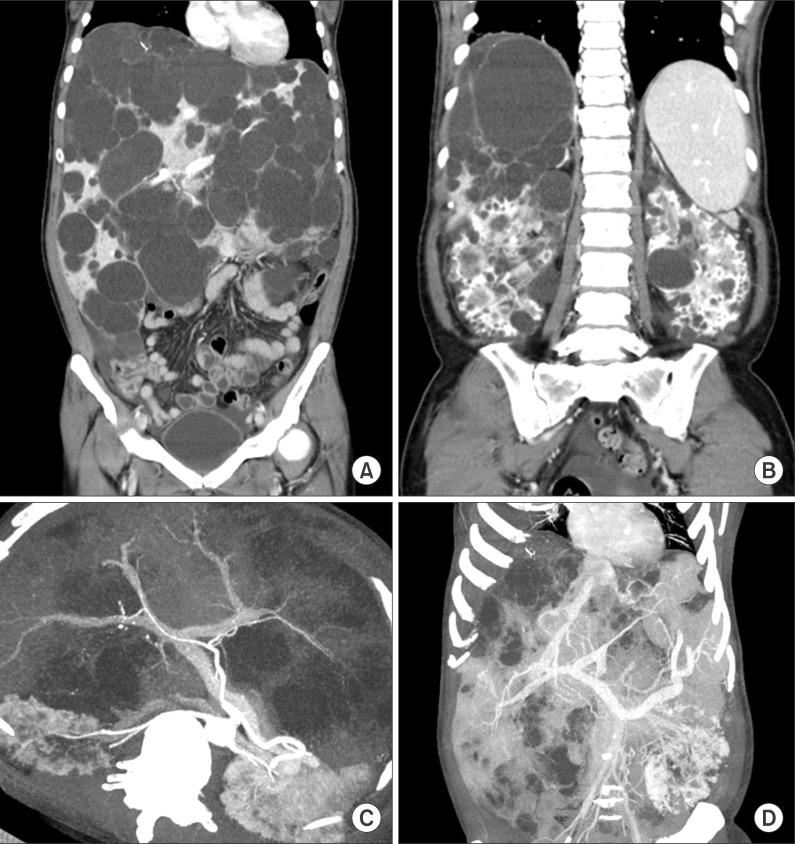
Fig. 1 Computed tomography images of the abdomen. Multiple cysts occupied the liver (A) and both kidneys (B), but the hepatic arterial and portal venous flow was well preserved (C) and hepatic veins were extrinsically compressed (D).
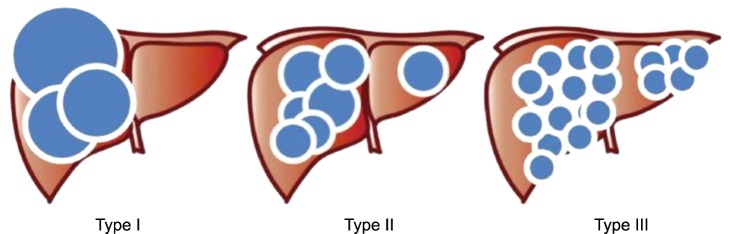
Fig. 2 Gross morphology of polycystic liver disease according to Gigot's classification. Type I: presence of less than 10 large hepatic cysts measuring more than 10 cm in maximum diameter. Type II: diffuse involvement of liver parenchyma by multiple cysts with remaining large areas of non-cystic liver parenchyma. Type III: presence of diffuse involvement of liver parenchyma by small- and medium-sized liver cysts with only a few areas of normal liver parenchyma.
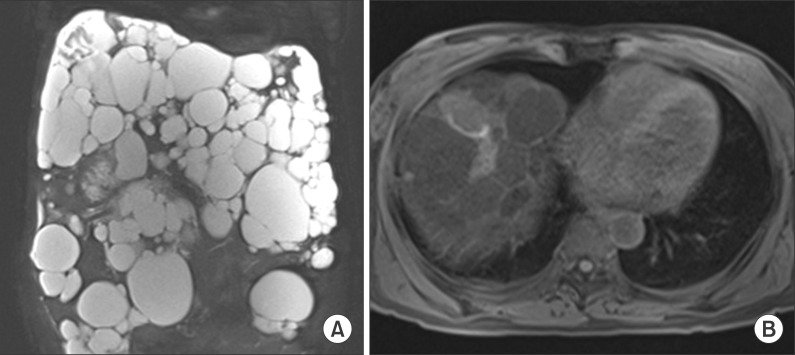
Fig. 3 Magnetic resonance imaging study of the abdomen. Waterfilled multiple liver and kidney cysts were visible (A). The gallbladder was collapsed by the adjacent liver cysts but the bile duct was not dilated (B).
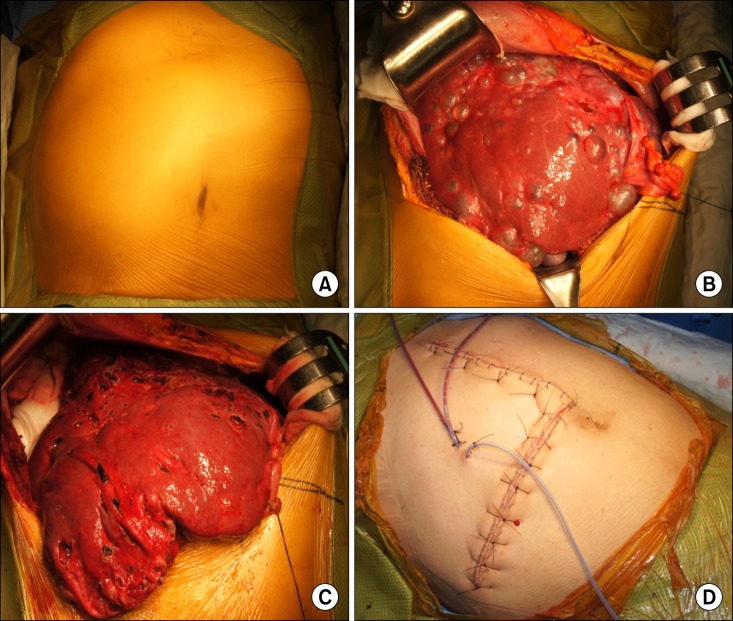
Fig. 4 Operative findings of the patient undergoing open fenestration surgery. Enlarged liver was bulged out of the abdomen (A); There were numerous liver cysts, but the majority of liver parenchyma was preserved (B); Fenestration of the liver cyst led to moderate reduction of the whole liver volume (C); Bulging mass in the abdomen disappeared at the time of abdominal wall closure (D).
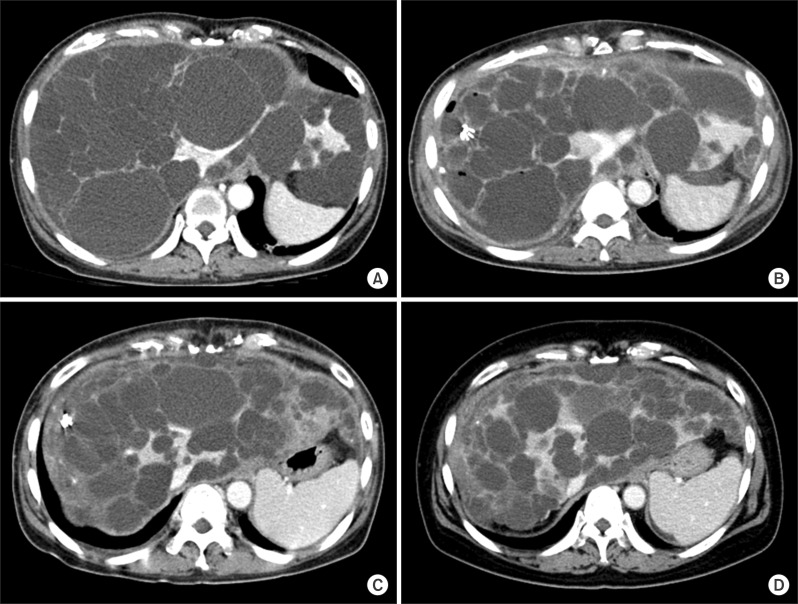
Fig. 5 Computed tomography follow-up of the abdomen. Multiple distended cysts occupied the liver just before surgery (A); Cyst size was significantly reduced 1 week after fenestration surgery (B); No increase in the size of liver cysts was observed in the 6-month (C) and 18-month (D) images. Because of improvement in the nutritional status, subcutaneous fat was thickened in the 18-month image (D).
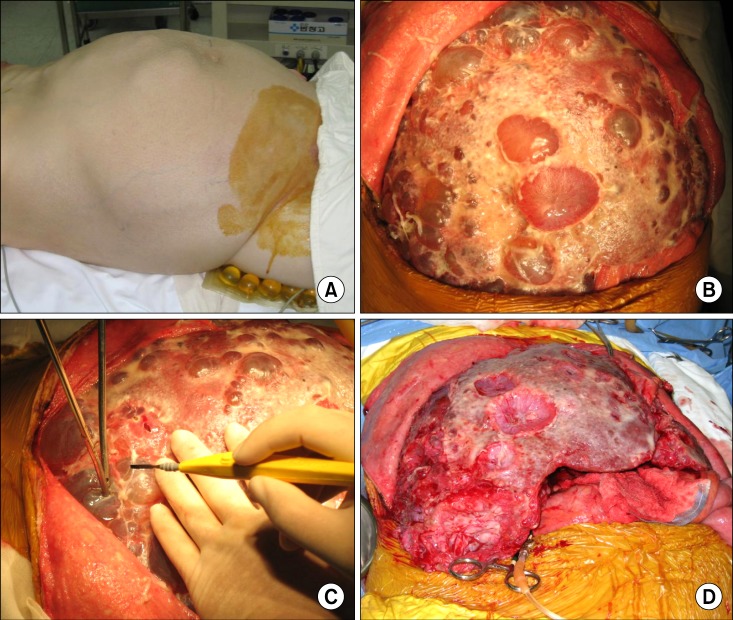
Fig. 6 Operative findings of a 52-year-old female patient undergoing liver transplantation with a MELD score of 18. Markedly enlarged liver was bulged out of the abdomen (A); There were numerous liver cysts that occupied the majority of liver parenchyma (B); Rupture of the liver cysts led to reduction of the liver volume (C), which facilitated handling of the native liver for liver transplantation (D).
Reference
-
1. Qian Q, Li A, King BF, Kamath PS, Lager DJ, Huston J 3rd, et al. Clinical profile of autosomal dominant polycystic liver disease. Hepatology. 2003; 37:164–171. PMID: 12500201.
Article2. Arnold HL, Harrison SA. New advances in evaluation and management of patients with polycystic liver disease. Am J Gastroenterol. 2005; 100:2569–2582. PMID: 16279915.
Article3. Szabó LS, Takács I, Arkosy P, Sápy P, Szentkereszty Z. Laparoscopic treatment of nonparasitic hepatic cysts. Surg Endosc. 2006; 20:595–597. PMID: 16437277.
Article4. van Keimpema L, Ruurda JP, Ernst MF, van Geffen HJ, Drenth JP. Laparoscopic fenestration of liver cysts in polycystic liver disease results in a median volume reduction of 12.5%. J Gastrointest Surg. 2008; 12:477–482. PMID: 17957434.
Article5. Everson GT, Taylor MR, Doctor RB. Polycystic disease of the liver. Hepatology. 2004; 40:774–782. PMID: 15382167.
Article6. Lin TY, Chen CC, Wang SM. Treatment of non-parasitic cystic disease of the liver: a new approach to therapy with polycystic liver. Ann Surg. 1968; 168:921–927. PMID: 5684196.7. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982; 5:649–655. PMID: 7165009.
Article8. Eypasch E, Williams JI, Wood-Dauphinee S, Ure BM, Schmülling C, Neugebauer E, et al. Gastrointestinal Quality of Life Index: development, validation and application of a new instrument. Br J Surg. 1995; 82:216–222. PMID: 7749697.
Article9. Gigot JF, Jadoul P, Que F, Van Beers BE, Etienne J, Horsmans Y, et al. Adult polycystic liver disease: is fenestration the most adequate operation for long-term management? Ann Surg. 1997; 225:286–294. PMID: 9060585.10. Qian Q, Li A, King BF, Kamath PS, Lager DJ, Huston J 3rd, et al. Clinical profile of autosomal dominant polycystic liver disease. Hepatology. 2003; 37:164–171. PMID: 12500201.
Article11. Schnelldorfer T, Torres VE, Zakaria S, Rosen CB, Nagorney DM. Polycystic liver disease: a critical appraisal of hepatic resection, cyst fenestration, and liver transplantation. Ann Surg. 2009; 250:112–118. PMID: 19561475.12. Gigot JF, Legrand M, Hubens G, de Canniere L, Wibin E, Deweer F, et al. Laparoscopic treatment of nonparasitic liver cysts: adequate selection of patients and surgical technique. World J Surg. 1996; 20:556–561. PMID: 8661625.
Article13. Giuliante F, D'Acapito F, Vellone M, Giovannini I, Nuzzo G. Risk for laparoscopic fenestration of liver cysts. Surg Endosc. 2003; 17:1735–1738. PMID: 12802647.
Article14. Konstadoulakis MM, Gomatos IP, Albanopoulos K, Alexakis N, Leandros E. Laparoscopic fenestration for the treatment of patients with severe adult polycystic liver disease. Am J Surg. 2005; 189:71–75. PMID: 15701496.
Article15. Robinson TN, Stiegmann GV, Everson GT. Laparoscopic palliation of polycystic liver disease. Surg Endosc. 2005; 19:130–132. PMID: 15531969.
Article16. Abu-Wasel B, Walsh C, Keough V, Molinari M. Pathophysiology, epidemiology, classification and treatment options for polycystic liver diseases. World J Gastroenterol. 2013; 19:5775–5786. PMID: 24124322.
Article17. Drenth JP, Chrispijn M, Nagorney DM, Kamath PS, Torres VE. Medical and surgical treatment options for polycystic liver disease. Hepatology. 2010; 52:2223–2230. PMID: 21105111.18. Que F, Nagorney DM, Gross JB Jr, Torres VE. Liver resection and cyst fenestration in the treatment of severe polycystic liver disease. Gastroenterology. 1995; 108:487–494. PMID: 7835591.
Article19. Everson GT, Taylor MR, Doctor RB. Polycystic disease of the liver. Hepatology. 2004; 40:774–782. PMID: 15382167.
Article20. Freeman RB Jr, Gish RG, Harper A, Davis GL, Vierling J, Lieblein L, et al. Model for end-stage liver disease (MELD) exception guidelines: results and recommendations from the MELD Exception Study Group and Conference (MESSAGE) for the approval of patients who need liver transplantation with diseases not considered by the standard MELD formula. Liver Transpl. 2006; 12:S128–S136. PMID: 17123284.
Article21. Arrazola L, Moonka D, Gish RG, Everson GT. Model for end-stage liver disease (MELD) exception for polycystic liver disease. Liver Transpl. 2006; 12:S110–S111. PMID: 17123287.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Polycystic liver disease: an overview of clinical manifestations, diagnosis, and treatment
- Surgical Treatment of Unilobar Adult Polycystic Liver Disease
- Living donor liver transplantation for huge polycystic liver disease with recipient liver splitting method: a case report
- Portal vein fenestration: a case report of an unusual portal vein developmental anomaly
- A Case Report of Renal Cell Carcinoma in a Polycystic Kidney: A case report
