Ectopic Insertion of the Pectoralis Minor Tendon: Inter-Reader Agreement and Findings in the Rotator Interval on MRI
- Affiliations
-
- 1Department of Radiology, Asan Foundation, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung 210-711, Korea. sjchoi@gnah.co.kr
- KMID: 1794648
- DOI: http://doi.org/10.3348/kjr.2014.15.6.764
Abstract
OBJECTIVE
To evaluate magnetic resonance imaging (MRI) observer variability to detect ectopic insertion of the pectoralis minor tendon (EIPMT) and to investigate changes in the rotator interval in patients with EIPMT using MRI.
MATERIALS AND METHODS
A total of 507 shoulder MRIs (male:female = 259:248; mean age, 55.4 years) were classified into 1) normal type insertion of the pectoralis minor tendon, 2) complete type EIPMT, and 3) partial type EIPMT independently by two radiologists. Inter-observer agreement was calculated using the kappa coefficient. Thickness of the fibrotic scar tissue in the subcoracoid triangle and humeral side axillary recess was measured. MRIs were reviewed by consensus with regard to the grade of fibrotic scar tissue proliferation in the rotator interval. Comparisons were made between normal and EIPMT and between partial and complete type EIPMT.
RESULTS
The incidence of EIPMT was 13.4% (complete type, 7.7%; partial type, 5.7%). Inter-observer agreement was substantial (kappa = 0.775). Fibrotic scar tissue in the subcoracoid triangle was thicker, and the grade of fibrotic scar tissue proliferation in the rotator interval was higher in the EIPMT group than those in the control group. No significant difference was observed in the thickness of humeral side axillary recess. The thicknesses of fibrotic scar tissue in the subcoracoid triangle and humeral side axillary recess as well as the grade of fibrotic scar tissue in the rotator interval were not significantly different between complete and partial type EIPMT.
CONCLUSION
MRI enabled detection of EIPMT with substantial observer agreement. Patients with EIPMT show a high tendency for fibrotic scar tissue proliferation in the rotator interval.
MeSH Terms
Figure
-
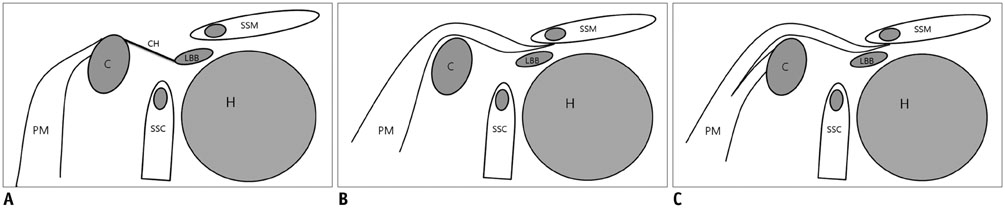
Fig. 1 Schematic diagram of insertion of pectoralis minor tendon (oblique sagittal images). A. Normal type insertion of pectoralis minor tendon into coracoid process. B. Complete type ectopic insertion of pectoralis minor tendon (EIPMT). Pectoralis minor tendon is passing over coracoid process without inserting into coracoid process (Le Double type 1). C. Partial type EIPMT. Pectoralis minor tendon has some portion normally inserted into coracoid process as well as another portion with anomalous insertion passing over coracoid process (Le Double type II). C = coracoid process, CH = coracohumeral ligament, H = humeral head, LBB = long head of biceps brachii, PM = pectoralis minor muscle and tendon, SSC = subscapularis muscle, SSM = supraspinatus muscle

Fig. 2 Schematic diagram of image analysis. A, B. Oblique sagittal images. Subcoracoid triangle (marked with asterisk in A). Borders of subcoracoid triangle were 1) coracoid process anterosuperiorly, 2) coracohumeral ligament in normal type cases (A) or pectoralis minor tendon passing over coracoid process in ectopic insertion of pectoralis minor tendon (EIPMT) cases (B) superiorly, and 3) joint capsule posteroinferiorly. Thickness (marked with double arrow) of fibrotic scar tissue (marked with gray color in subcoracoid triangle) was measured in subcoracoid triangle adjacent to coracoid process. Degree of fibrotic scar tissue proliferation was graded according to occupying area of fibrotic scar tissue in rotator interval and subcoracoid area. C. Coronal image. Thickness of humeral axillary recess was measured at widest portion (marked with double arrow) of capsule and axillary recess synovium perpendicular to adjacent cortical bone of humeral neck. AR = axillary recess, C = coracoid process, CH = coracohumeral ligament, H = humeral head, JC = joint capsule, L = labrum, LBB = long head of biceps brachii, PM = pectoralis minor muscle and tendon, SSC = subscapularis muscle, SSM = supraspinatus muscle
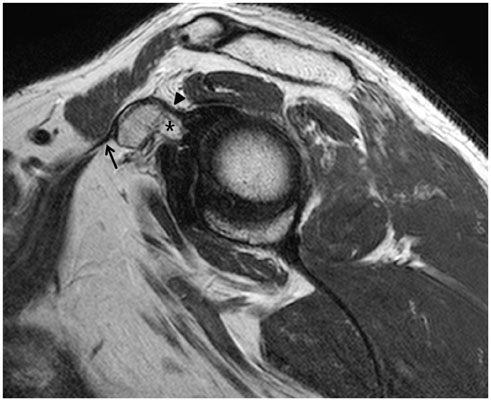
Fig. 3 Left shoulder magnetic resonance image of 47-year-old man with normal type insertion of pectoralis minor tendon. Oblique sagittal T2-weighted image shows pectoralis minor tendon (arrow) inserting into anterior aspect of coracoid process. Note that coracohumeral ligament (arrowhead) originated separately from superior aspect of coracoid process. No definite fibrotic scar tissue proliferation (marked with asterisk) in subcoracoid triangle and rotator interval was detected.
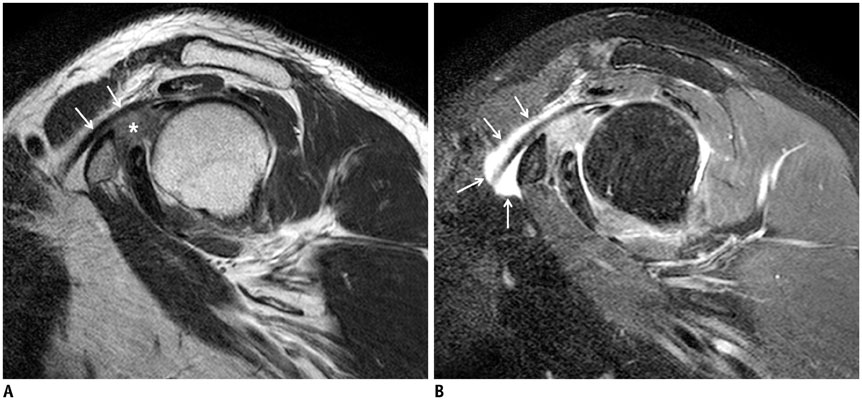
Fig. 4 Right shoulder magnetic resonance image of 60-year-old man with complete type ectopic insertion of pectoralis minor tendon (EIPMT). A. Oblique sagittal T2-weighted image shows pectoralis minor tendon (arrows) passing over coracoid process. Note severe degree of fibrotic scar tissue proliferation in subcoracoid area and rotator interval (marked with asterisk). B. Oblique sagittal T2 spectral adiabatic inversion recovery image shows fluid collection (marked with arrows) along pectoralis minor tendon extending over coracoid process. Fluid might be communicating with glenohumoral joint in this case of complete type EIPMT.

Fig. 5 Left shoulder magnetic resonance image of 58-year-old woman with partial type ectopic insertion of pectoralis minor tendon. A-C. Sequential oblique sagittal T2-weighted images show pectoralis minor tendon slip (arrows) passing over coracoid process and running underneath supraspinatus muscle, while main portion of pectoralis minor tendon (arrowheads in A and B) inserts into anterior aspect of coracoid process. Note moderate degree of fibrotic scar tissue proliferation (marked with asterisk in C) in subcoracoid area including rotator interval.
Reference
-
1. Le Double AF. Traité des variations du système musculaire de l'homme et de leur signification au point de vue de l'anthropologie zoologique. Paris: Schleicher frères;1897. p. 252–255.2. Weinstabl R, Hertz H, Firbas W. [Connection of the ligamentum coracoglenoidale with the muscular pectoralis minor]. Acta Anat (Basel). 1986; 125:126–113.3. Homsi C, Rodrigues MB, Silva JJ, Stump X, Morvan G. [Anomalous insertion of the pectoralis minor muscle: ultrasound findings]. J Radiol. 2003; 84:1007–1011.4. Samuel P, Blanchard JP. [Rotator cuff syndrome caused by an anomaly of the insertion of the pectoralis minor]. Rev Chir Orthop Reparatrice Appar Mot. 1984; 70:401–404.5. Hatakeyama Y, Itoi E, Urayama M, Pradhan RL, Sato K. Effect of superior capsule and coracohumeral ligament release on strain in the repaired rotator cuff tendon. A cadaveric study. Am J Sports Med. 2001; 29:633–664.6. Apoil A. [Antero-internal impingement of the shoulder]. Ann Radiol (Paris). 1992; 35:161–116.7. Dumontier C, Sautet A, Gagey O, Apoil A. Rotator interval lesions and their relation to coracoid impingement syndrome. J Shoulder Elbow Surg. 1999; 8:130–135.8. Moineau G, Cikes A, Trojani C, Boileau P. Ectopic insertion of the pectoralis minor: implication in the arthroscopic treatment of shoulder stiffness. Knee Surg Sports Traumatol Arthrosc. 2008; 16:869–871.9. Yoo JC, Lim TK, Koh KH, Park WH. Arthroscopic perspective of the tendinous insertion of the pectoralis minor and correlation with MRI: a case report. J Shoulder Elbow Surg. 2010; 19:e19–e23.10. Lee SJ, Ha DH, Lee SM. Unusual variation of the rotator interval: insertional abnormality of the pectoralis minor tendon and absence of the coracohumeral ligament. Skeletal Radiol. 2010; 39:1205–1209.11. Low SC, Tan SC. Ectopic insertion of the pectoralis minor muscle with tendinosis as a cause of shoulder pain and clicking. Clin Radiol. 2010; 65:254–256.12. Uzel AP, Bertino R, Caix P, Boileau P. Bilateral variation of the pectoralis minor muscle discovered during practical dissection. Surg Radiol Anat. 2008; 30:679–682.13. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33:159–174.14. Emig EW, Schweitzer ME, Karasick D, Lubowitz J. Adhesive capsulitis of the shoulder: MR diagnosis. AJR Am J Roentgenol. 1995; 164:1457–1459.15. Mengiardi B, Pfirrmann CW, Gerber C, Hodler J, Zanetti M. Frozen shoulder: MR arthrographic findings. Radiology. 2004; 233:486–492.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Variant pectoralis minor muscle: a case study with clinical relevance
- Tendon Transfer for Irreparable Massive Rotator Cuff Tear
- Visual MRI Grading System to Evaluate Atrophy of the Supraspinatus Muscle
- The Association between the Magnetic Resonance Imaging Findings of Adhesive Capsulitis and Shoulder Muscle Fat Quantification Using a Multi-Echo Dixon Method
- Biological Characteristics of Rotator Cuff Tendon
