Solid Pancreatic Tumors with Unilocular Cyst-Like Appearance on CT: Differentiation from Unilocular Cystic Tumors Using CT
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea. jhbyun@amc.seoul.kr
- 2Department of Radiology, National Cancer Center, Goyang 410-769, Korea.
- KMID: 1794641
- DOI: http://doi.org/10.3348/kjr.2014.15.6.704
Abstract
OBJECTIVE
To describe the computed tomography (CT) features of neuroendocrine tumors (NETs) and solid pseudopapillary tumors (SPTs) with unilocular cyst-like appearance, and to compare them with those of unilocular cystic tumors of the pancreas.
MATERIALS AND METHODS
This retrospective study was approved by our Institutional Review Board, and informed consent was waived. We included 112 pancreatic tumors with unilocular cyst-like appearance on CT (16 solid tumors [nine NETs and seven SPTs] and 96 cystic tumors [45 serous cystadenomas, 30 mucinous cystic neoplasms, and 21 branch-duct intraductal papillary mucinous neoplasms]). Two radiologists reviewed the CT images in consensus to determine tumor location, long diameter, morphological features, wall thicknesses, ratio of wall thickness to tumor size, wall enhancement patterns, intratumoral contents, and accompanying findings. Fisher's exact test was used to analyze the results.
RESULTS
All 16 solid tumors had perceptible walls (mean thickness, 2.7 mm; mean ratio of wall thickness to tumor size, 7.7%) with variable enhancement. Four NETs and seven SPTs had hemorrhage, calcifications, and/or mural nodules. Six CT findings were specific for solid tumors with unilocular cyst-like appearance: a thick (> 2 mm) wall, uneven thickness of the wall, high ratio of wall thickness to tumor size, hyper- or hypo-attenuation of the wall in the arterial and portal phase, and heterogeneous internal contents. When three or more of the above criteria were used, 100% specificity and 87.5-92% accuracy were obtained for solid tumors with unilocular cyst-like appearance.
CONCLUSION
A combination of CT features was useful for distinguishing solid tumors with unilocular cyst-like appearance from unilocular cystic tumors of the pancreas.
Keyword
MeSH Terms
-
Adenocarcinoma, Mucinous/diagnosis/*radiography
Adult
Aged
Carcinoma, Papillary/diagnosis/*radiography
Cystadenoma, Serous
Diagnosis, Differential
Female
Humans
Male
Middle Aged
Neuroendocrine Tumors/diagnosis/*radiography
Pancreatic Neoplasms/diagnosis/*radiography
Retrospective Studies
Sensitivity and Specificity
Tomography, X-Ray Computed
Figure
-
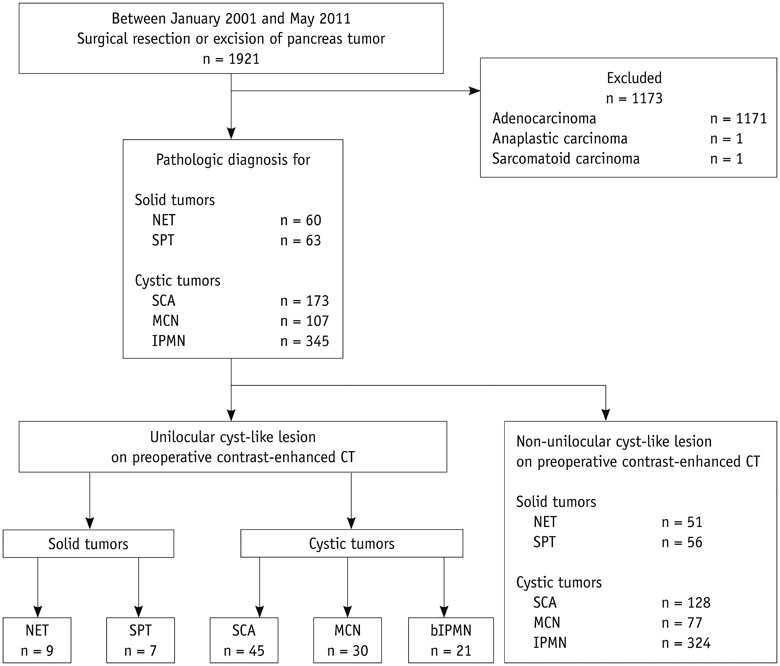
Fig. 1 Flow diagram of study patients. Data are numbers of tumors. bIPMN = branch-duct intraductal papillary mucinous neoplasm, MCN = mucinous cystic neoplasm, NET = neuroendocrine tumor, SCA = serous cystadenoma, SPT = solid pseudopapillary tumor

Fig. 2 Pancreatic neuroendocrine tumor in 54-year-old woman. A, B. Transverse contrast-enhanced arterial (A) and portal (B) phase computed tomography images demonstrate 2-cm round cyst-like mass in pancreatic tail. Thick (3.3 mm) uneven wall (white arrows) shows high attenuation in arterial phase and iso-attenuation in portal phase.
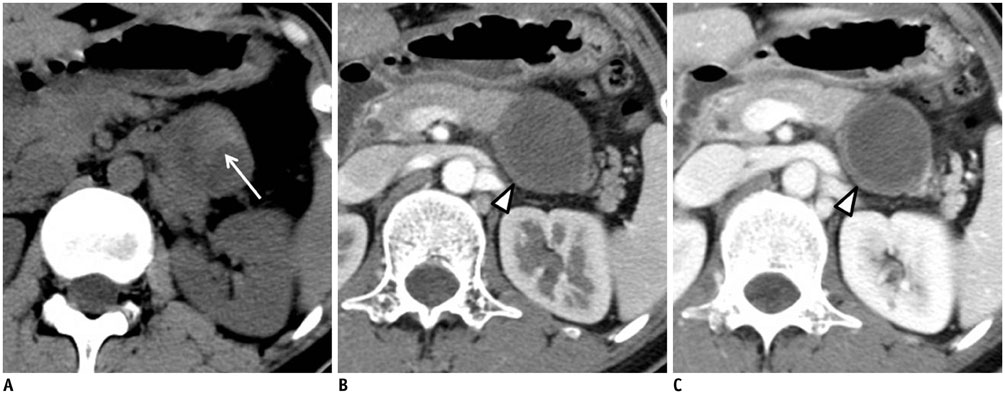
Fig. 3 Solid pseudopapillary tumor in 33-year-old-woman. A. Transverse precontrast computed tomography (CT) image shows 3.5-cm round mass with intratumoral high attenuated lesions (white arrow), suggesting internal hemorrhage. B, C. Transverse contrast-enhanced arterial (B) and portal (C) phase CT images show unilocular cyst-like mass with low-attenuating, thick (3.4 mm) uneven wall (white arrowheads).
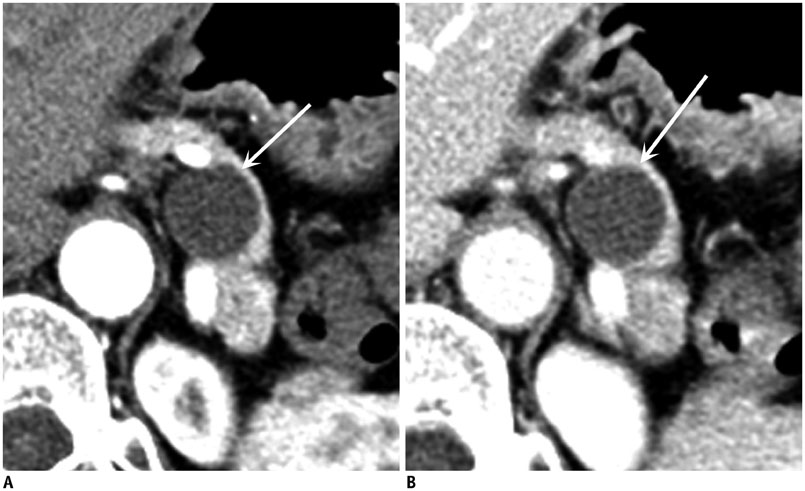
Fig. 4 Mucinous cystadenoma in 54-year-old woman. A, B. Transverse contrast-enhanced arterial (A) and portal (B) phase computed tomography images demonstrate 2.3-cm round cystic mass (white arrows) in pancreatic tail. Even thin (1 mm) wall shows iso-attenuation in arterial and portal phases.
Cited by 1 articles
-
What Is New in the 2017 World Health Organization Classification and 8th American Joint Committee on Cancer Staging System for Pancreatic Neuroendocrine Neoplasms?
Jooae Choe, Kyung Won Kim, Hyoung Jung Kim, Dong Wook Kim, Kyu Pyo Kim, Seung-Mo Hong, Jin-Sook Ryu, Sree Harsha Tirumani, Katherine Krajewski, Nikhil Ramaiya
Korean J Radiol. 2019;20(1):5-17. doi: 10.3348/kjr.2018.0040.
Reference
-
1. Fernández-del Castillo C, Warshaw AL. Cystic tumors of the pancreas. Surg Clin North Am. 1995; 75:1001–1016.2. Sidden CR, Mortele KJ. Cystic tumors of the pancreas: ultrasound, computed tomography, and magnetic resonance imaging features. Semin Ultrasound CT MR. 2007; 28:339–356.3. Warshaw AL, Rutledge PL. Cystic tumors mistaken for pancreatic pseudocysts. Ann Surg. 1987; 205:393–398.4. Tipton SG, Smyrk TC, Sarr MG, Thompson GB. Malignant potential of solid pseudopapillary neoplasm of the pancreas. Br J Surg. 2006; 93:733–737.5. Bordeianou L, Vagefi PA, Sahani D, Deshpande V, Rakhlin E, Warshaw AL, et al. Cystic pancreatic endocrine neoplasms: a distinct tumor type? J Am Coll Surg. 2008; 206:1154–1158.6. Tan G, Vitellas K, Morrison C, Frankel WL. Cystic schwannoma of the pancreas. Ann Diagn Pathol. 2003; 7:285–291.7. Ahrendt SA, Komorowski RA, Demeure MJ, Wilson SD, Pitt HA. Cystic pancreatic neuroendocrine tumors: is preoperative diagnosis possible? J Gastrointest Surg. 2002; 6:66–74.8. Warshaw AL, Compton CC, Lewandrowski K, Cardenosa G, Mueller PR. Cystic tumors of the pancreas. New clinical, radiologic, and pathologic observations in 67 patients. Ann Surg. 1990; 212:432–443. discussion 444-445.9. Volkan Adsay N. Cystic lesions of the pancreas. Mod Pathol. 2007; 20:S71–S93.10. Cohen-Scali F, Vilgrain V, Brancatelli G, Hammel P, Vullierme MP, Sauvanet A, et al. Discrimination of unilocular macrocystic serous cystadenoma from pancreatic pseudocyst and mucinous cystadenoma with CT: initial observations. Radiology. 2003; 228:727–733.11. Adsay NV, Klimstra DS. Cystic forms of typically solid pancreatic tumors. Semin Diagn Pathol. 2000; 17:81–88.12. Klimstra DS, Wenig BM, Heffess CS. Solid-pseudopapillary tumor of the pancreas: a typically cystic carcinoma of low malignant potential. Semin Diagn Pathol. 2000; 17:66–80.13. Singhal D, Kakodkar R, Sud R, Chaudhary A. Issues in management of pancreatic pseudocysts. JOP. 2006; 7:502–507.14. Sahani DV, Kadavigere R, Saokar A, Fernandez-del Castillo C, Brugge WR, Hahn PF. Cystic pancreatic lesions: a simple imaging-based classification system for guiding management. Radiographics. 2005; 25:1471–1484.15. Scott J, Martin I, Redhead D, Hammond P, Garden OJ. Mucinous cystic neoplasms of the pancreas: imaging features and diagnostic difficulties. Clin Radiol. 2000; 55:187–192.16. Kim SY, Lee JM, Kim SH, Shin KS, Kim YJ, An SK, et al. Macrocystic neoplasms of the pancreas: CT differentiation of serous oligocystic adenoma from mucinous cystadenoma and intraductal papillary mucinous tumor. AJR Am J Roentgenol. 2006; 187:1192–1198.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pancreatic Tumors: Emphasis on CT Findings and Pathologic Classification
- Cystic Thymic Diseases: CT Manifestations
- Ameloblastoma of the Mandible and Maxilla: CT Findings
- Radiologic Findings of the Serous Cystadenomas of the Pancreas with Macro cystic or Unilocular Variants: Comparison with the Pathologic Findings
- Radiologic Findings of Granulosa Cell Tumor of the Ovary
