Pancreatic Tumors: Emphasis on CT Findings and Pathologic Classification
- Affiliations
-
- 1Department of Radiology and the Research Institute of Radiological Sciences, Severance Hospital, Yonsei University College of Medicine, Seoul 120-752, Korea. gafield2@yuhs.ac
- KMID: 1101928
- DOI: http://doi.org/10.3348/kjr.2011.12.6.731
Abstract
- Pancreatic tumors can be classified by their morphologic features on CT. The subtypes include solid tumors, mixed cystic and solid lesions, unilocular cysts, multilocular cystic lesions, and microcystic lesions. Endoscopic US and MRI can provide detailed information for classifying pancreatic lesions. Each subtype has different kinds of tumors and malignant potential, thus the classification can be useful for a better differential diagnosis and treatment planning. For this purpose, we suggest an appropriate modified classification system by using the imaging features of pancreatic tumors with an emphasis on CT findings and illustrate various findings of typical and atypical manifestations.
Keyword
MeSH Terms
Figure
-
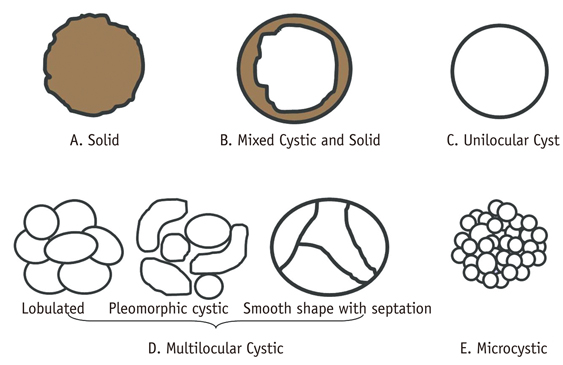
Fig. 1 Morphologic subtypes of pancreatic lesions. Because each pancreatic neoplasm has different malignant potential, it is clinically valuable to determine characteristic imaging findings that can enable differentiation. We classified pancreatic tumors into solid tumors (A malignant or potentially malignant), mixed cystic and solid lesions (B malignant or potentially malignant), unilocular cysts (C benign or potentially malignant), multilocular cystic lesions (D benign or potentially malignant), and microcystic lesions (E benign). Multilocular cystic lesions are divided into three categories including lobulated (benign), pleomorphic (from benign to malignant), and smooth in shape with septation (potentially malignant). These figures are made by referring to previously suggested classification schema (5).
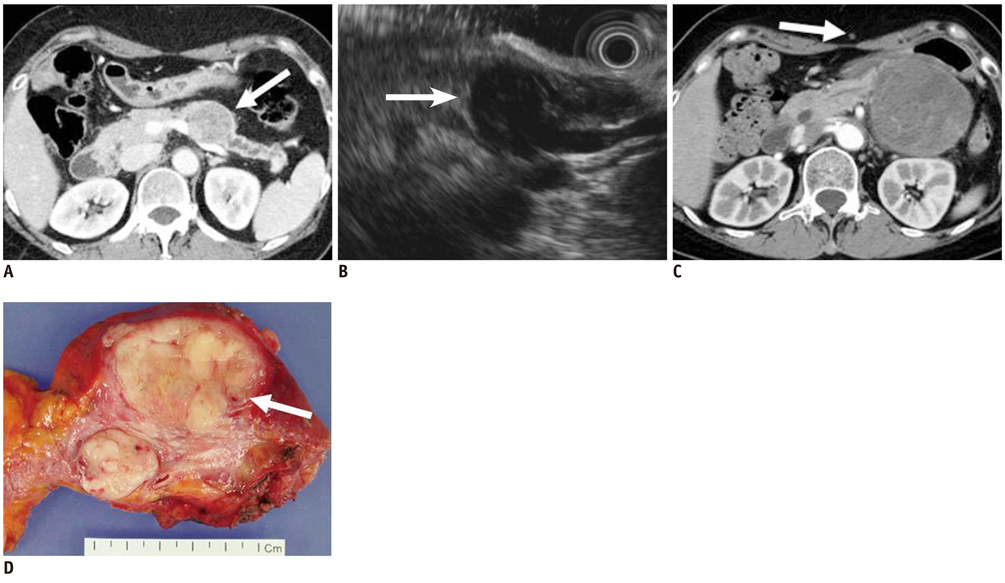
Fig. 2 58-year-old woman with metastatic leiomyosarcoma manifesting as solid lesion. A. Contrast-enhanced CT image during venous phase shows well-marginated, low attenuating solid tumor in pancreas (white arrow). B. Endoscopic US image depicts heterogeneously hypoechoic solid tumor (white arrow). Woman had multiple painless metastatic tumors in her stomach, chest, thigh and pancreas, which were too numerous to excise. Consequently, surgery was ruled out, and only chemotherapy was performed. C. Woman began to feel sick and mass increased in size at 1-year follow-up CT. Note metastatic nodule in subcutaneous layer (white arrow). D. Tumor was finally excised and appeared as whitish solid tumor in gross specimen and was confirmed as metastatic leiomyosarcoma (white arrow).
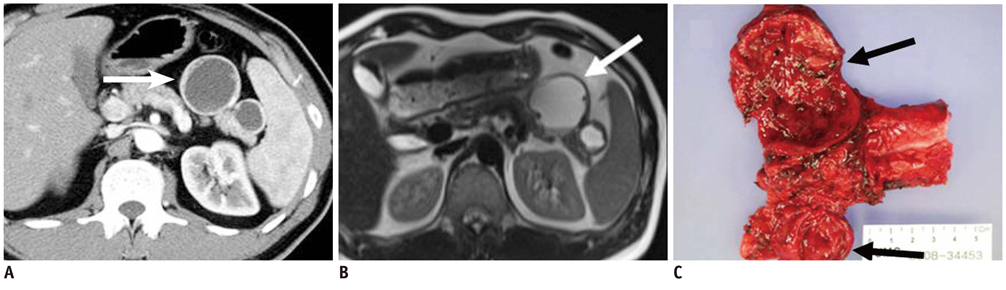
Fig. 3 40-year-old man with cystic change of islet cell tumor manifesting as mixed cystic and solid lesion. A. Contrast enhanced CT image during arterial phase shows two unilocular cystic lesions with small solid components in tail of pancreas (white arrow). B. T2-weighted image shows cystic character of lesions (white arrow). C. Surgical specimen shows two predominantly cystic lesions with solid portion and small mural nodules. Microscopic examination revealed cystic change of islet cell tumors (black arrows).
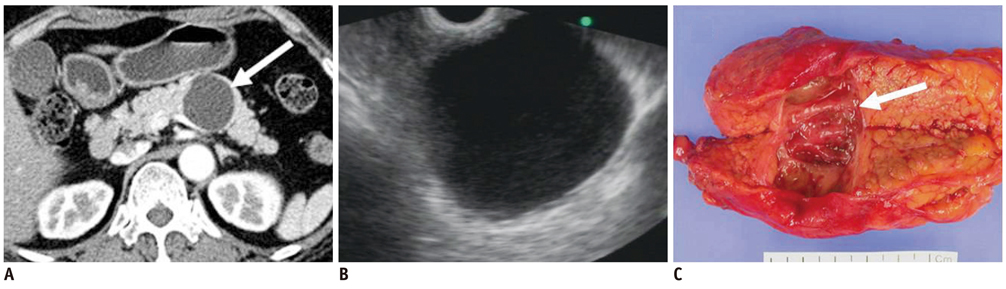
Fig. 4 57-year-old woman with mucinous cystic neoplasm manifesting as unilocular cyst. A. Transverse contrast enhanced CT image during arterial phase shows unilocular cyst (white arrow) in body of pancreas. B. Endoscopic US image depicts cyst without solid portion or septation. C. Gross specimen reveals unilocular cystic lesions without septation or solid mural nodule (white arrow). Communication with pancreatic duct was not found. Tumor was confirmed as mucinous cystadenoma.
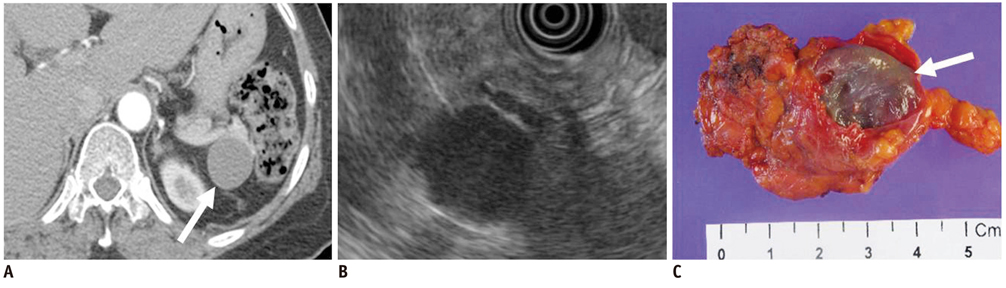
Fig. 5 47-year-old woman with lymphoepithelial cyst manifesting as unilocular cyst. A. Transverse contrast enhanced CT image during arterial phase shows unilocular cystic lesion in tail of pancreas (white arrow). B. Endoscopic US image shows homogeneous echoic cystic lesion. C. Surgical specimen shows round tumor with surrounding fibrous capsule (white arrow).
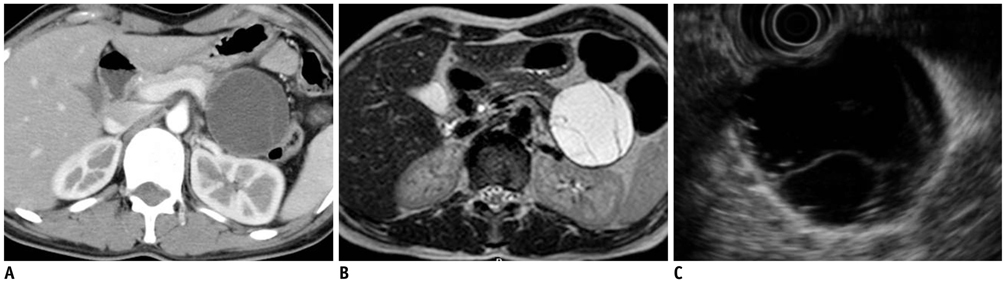
Fig. 6 27-year-old woman with mucinous cystic neoplasm manifesting as multilocular cystic lesion (smooth shape with septation). A. Contrast enhanced CT image during venous phase obtained after intravenous injection of contrast material reveals smooth-shaped cystic lesion in tail of pancreas. B. Axial T2-weighted MR image reveals multiple internal septa in cystic lesion. C. Endoscopic US image also depicts multilocular cystic lesion with smooth shape and multiple inner septa, which was consistent with mucinous cystic neoplasm.

Fig. 7 37-year-old woman with serous cystadenoma manifesting as multilocular cystic lesion (lobulated). A. Contrast-enhanced CT image during venous phase shows multilocular cyst in body of pancreas. Lobulated shape of tumor corresponds to polycystic serous cystadenoma rather than mucinous cystadenoma. B. Endoscopic US depicts tumor composed of multiple cysts. Endoscopic US-guided aspiration showed no malignant cell. C. Ill-defined multilocular cystic tumor with inner smooth and trabeculated surface is seen in gross specimen (white arrows) and confirmed as serous cystadenoma composed of variable sized cysts lined by simple cuboidal cells.

Fig. 8 43-year-old man with branch duct type intraductal papillary mucinous neoplasm manifesting as multilocular cystic lesion (pleomorphic cystic). A. Contrast enhanced CT image during venous phase shows multilocular pleomorphic cystic lesion in head of pancreas. B. Note dilated downstream pancreatic duct (black arrow). C. Gross specimen showing ill-defined multilocular cystic tumor in head of pancreas (black arrow) which contained mucinous material. Tumor connects with irregularly dilated branches of pancreatic duct, and is confirmed as branch duct type intraductal papillary mucinous neoplasm.
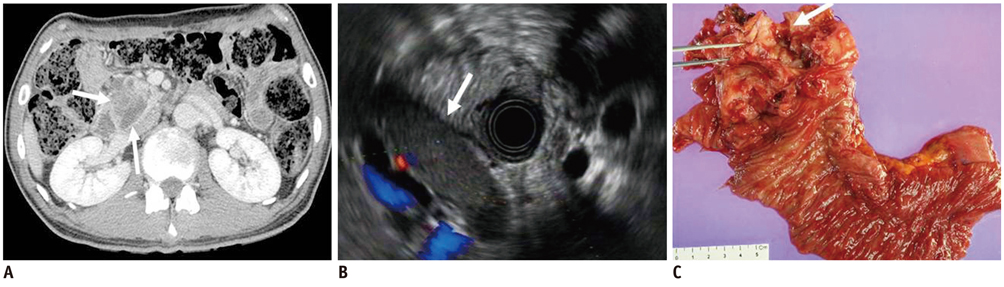
Fig. 9 52-year-old man with invasive intraductal papillary mucinous neoplasm. A. Contrast-enhanced CT image during venous phase shows dilatation of main pancreatic duct with adjacent solid mass in head of pancreas (white arrows). B. Endoscopic US image shows cystic lesion with inner solid portion (white arrow). C. Surgical specimen shows tumor involvement of dilated main pancreatic duct (white arrow). Microscopic examination revealing invasive intraductal papillary mucinous neoplasm.

Fig. 10 66-year-old man with microcystic serous cystadenoma manifesting as microcystic lesion. A. Contrast-enhanced transverse CT during arterial phase shows hypervascular mass (white arrow) in tail of pancreas. It appears as solid lesion on CT, owing to innumerable cysts and fine septa. B. Note cystic portion in periphery of tumor (white arrow). C. Axial T2-weighted image reveals microcystic mass. D. Gross specimen shows multilocular, well-defined bulging mass containing multiple tiny cystic spaces and sanguineous clear fluid (white arrow), which are confirmed as microcystic serous cystadenoma.
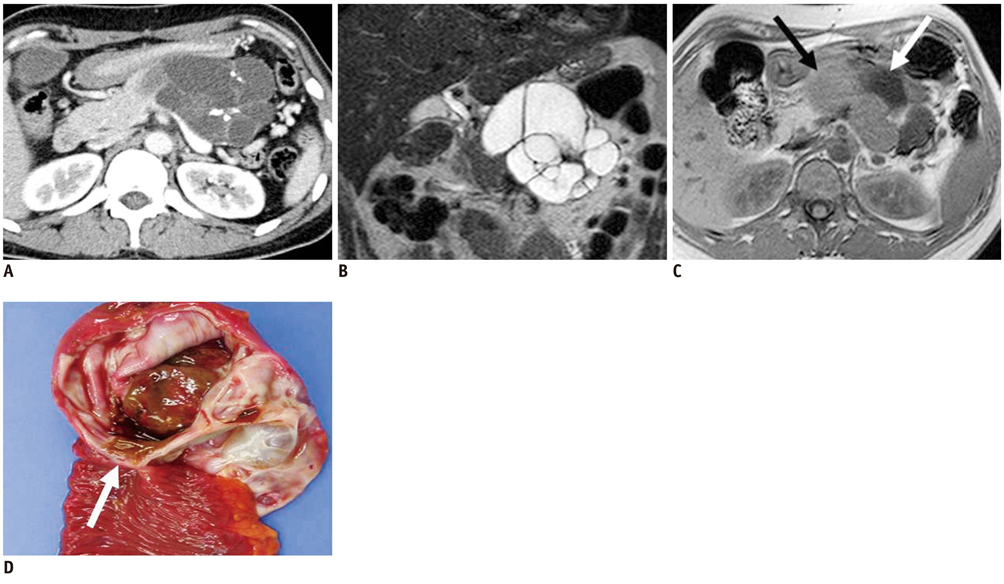
Fig. 11 37-year-old woman with mucinous cystic neoplasm: pitfall in differentiating multilocular cystic lesions. A. Contrast-enhanced CT image during venous phase shows multilocular lobulated cyst with internal septation and calcification in tail of pancreas. B. Coronal T2-weighted image reveals multilocular cystic mass. C. T1-weighted gradient-echo image shows multiple locules with different signal intensity (black and white arrows). D. Gross specimen shows multilocular cystic tumor with inner smooth and glistening surface (white arrow) which was confirmed as mucinous cystadenoma at microscopy.

Fig. 12 59-year-old-woman with branch duct type intraductal papillary mucinous neoplasm manifesting as mixed cystic and solid lesion. A. Contrast-enhanced CT image during venous phase shows cystic mass and internal solid portion in head of pancreas (white arrow). B. Two-dimensional thick slab MR cholangiopancreatography image shows cystic mass in head of pancreas. Communication between cystic mass and pancreatic duct is not clear. C. Source image of 3D-MR cholangiopancreatography shows narrow tumor neck suggesting communication between tumor and main pancreatic duct more clearly than 2D-MR cholangiopancreatography (white arrow). D. Gross specimen shows whitish polypoid friable mass containing translucent mucoid materials. Tumor communicates with main pancreatic duct (white arrow) and was confirmed as branch duct type intraductal papillary mucinous neoplasm.
Cited by 1 articles
-
Retroperitoneal Extraskeletal Osteosarcoma without Calcification Mimicking Pancreas Tumor: CT Imaging of a Case Report
Jung Won Kim, Kyung Eun Bae, Kyeong Mee Park, Jae Hyung Kim, Myeong Ja Jeong, Soung Hee Kim, Ji Young Kim, Soo Hyun Kim, Mi Jin Kang, Ji Hae Lee, Tae Gyu Kim
J Korean Soc Radiol. 2018;78(5):340-344. doi: 10.3348/jksr.2018.78.5.340.
Reference
-
1. Kim SY, Lee JM, Kim SH, Shin KS, Kim YJ, An SK, et al. Macrocystic neoplasms of the pancreas: CT differentiation of serous oligocystic adenoma from mucinous cystadenoma and intraductal papillary mucinous tumor. AJR Am J Roentgenol. 2006. 187:1192–1198.2. Park MS, Kim KW, Lim JS, Lee JH, Kim JH, Kim SY, et al. Unusual cystic neoplasms in the pancreas: radiologic-pathologic correlation. J Comput Assist Tomogr. 2005. 29:610–616.3. Irie H, Honda H, Aibe H, Kuroiwa T, Yoshimitsu K, Shinozaki K, et al. MR cholangiopancreatographic differentiation of benign and malignant intraductal mucin-producing tumors of the pancreas. AJR Am J Roentgenol. 2000. 174:1403–1408.4. Song SJ, Lee JM, Kim YJ, Kim SH, Lee JY, Han JK, et al. Differentiation of intraductal papillary mucinous neoplasms from other pancreatic cystic masses: comparison of multirow-detector CT and MR imaging using ROC analysis. J Magn Reson Imaging. 2007. 26:86–93.5. Sahani DV, Kadavigere R, Saokar A, Fernandez-del Castillo C, Brugge WR, Hahn PF. Cystic pancreatic lesions: a simple imaging-based classification system for guiding management. Radiographics. 2005. 25:1471–1484.6. Mergo PJ, Helmberger TK, Buetow PC, Helmberger RC, Ros PR. Pancreatic neoplasms: MR imaging and pathologic correlation. Radiographics. 1997. 17:281–301.7. Lee LY, Hsu HL, Chen HM, Hsueh C. Ductal adenocarcinoma of the pancreas with huge cystic degeneration: a lesion to be distinguished from pseudocyst and mucinous cystadenocarcinoma. Int J Surg Pathol. 2003. 11:235–239.8. Choi JY, Kim MJ, Kim JH, Kim SH, Lim JS, Oh YT, et al. Solid pseudopapillary tumor of the pancreas: typical and atypical manifestations. AJR Am J Roentgenol. 2006. 187:W178–W186.9. Cohen-Scali F, Vilgrain V, Brancatelli G, Hammel P, Vullierme MP, Sauvanet A, et al. Discrimination of unilocular macrocystic serous cystadenoma from pancreatic pseudocyst and mucinous cystadenoma with CT: initial observations. Radiology. 2003. 228:727–733.10. Curry CA, Eng J, Horton KM, Urban B, Siegelman S, Kuszyk BS, et al. CT of primary cystic pancreatic neoplasms: can CT be used for patient triage and treatment? AJR Am J Roentgenol. 2000. 175:99–103.11. Kawamoto S, Horton KM, Lawler LP, Hruban RH, Fishman EK. Intraductal papillary mucinous neoplasm of the pancreas: can benign lesions be differentiated from malignant lesions with multidetector CT? Radiographics. 2005. 25:1451–1468. discussion 1468-1470.12. Levy MJ, Clain JE. Evaluation and management of cystic pancreatic tumors: emphasis on the role of EUS FNA. Clin Gastroenterol Hepatol. 2004. 2:639–653.13. Brugge WR. The use of EUS to diagnose cystic neoplasms of the pancreas. Gastrointest Endosc. 2009. 69:S203–S209.14. Choi JY, Kim MJ, Lee JY, Lim JS, Chung JJ, Kim KW, et al. Typical and atypical manifestations of serous cystadenoma of the pancreas: imaging findings with pathologic correlation. AJR Am J Roentgenol. 2009. 193:136–142.15. Shintaku M, Arimoto A, Sakita N. Serous cystadenocarcinoma of the pancreas. Pathol Int. 2005. 55:436–439.16. Choi JY, Lee JM, Lee MW, Kim SJ, Choi SY, Kim JY, et al. Magnetic resonance pancreatography: comparison of two- and three-dimensional sequences for assessment of intraductal papillary mucinous neoplasm of the pancreas. Eur Radiol. 2009. 19:2163–2170.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Computed tomographic findings in posterior cranial fossa tumors: correlation between angiographic vascularityand CT enhancement
- CT in the diagnosis of pancreatic trauma
- Islet Cell Tumors of the Pancreas: A Variety of MultiphaseDynamic Imaging Findings with Pathologic Correlations Focusing on Nonfunctioning Tumors and Insulinomas
- Pathologic Features of Pancreatic Cystic Neoplasms
- Imaging Findings of Perineal Disease
