J Korean Soc Radiol.
2015 May;72(5):348-351. 10.3348/jksr.2015.72.5.348.
Massive Hemobilia due to Hepatic Arteriobiliary Fistula during Endoscopic Retrograde Cholangiopancreatography: An Extremely Rare Guidewire-Related Complication
- Affiliations
-
- 1Department of Radiology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. stent@paran.com
- 2Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- KMID: 1793892
- DOI: http://doi.org/10.3348/jksr.2015.72.5.348
Abstract
- Although endoscopic retrograde cholangiopancreatography (ERCP) is an effective modality for diagnosis and treatment of biliary and pancreatic diseases, the risk for procedure-related complications is high. Hemorrhage is one of major complications of ERCP. Most ERCP-associated bleeding is primarily a complication related to sphincterotomy rather than diagnostic ERCP. We are reporting a case of massive hemobilia due to hepatic arteriobiliary fistula caused by guidewire-associated injury during ERCP, which was successfully treated with transarterial embolization of the hepatic artery.
MeSH Terms
Figure
-
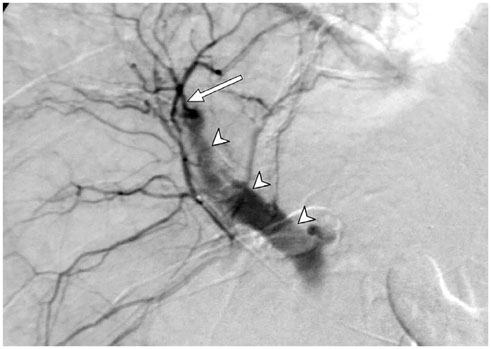
Fig. 1 Selective hepatic arteriography showed an arteriobiliary fistula (arrow) with active contrast extravasation into the bile duct (arrowheads).
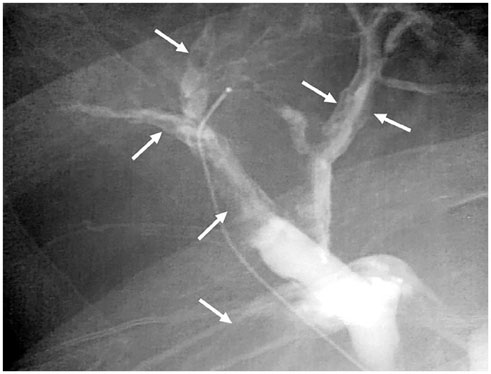
Fig. 2 Fluoroscopy following hepatic arteriography revealed irregular cast-like filling defects (arrows) in the bile duct due to massive hemobilia.
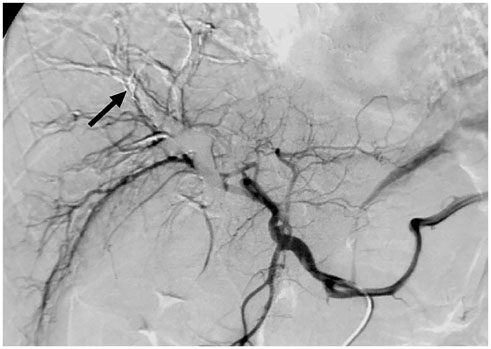
Fig. 3 Common hepatic arteriography after selective coil embolization showed coils (arrow) that were placed at the hepatic artery branch and no longer contrast extravasation.

Fig. 4 Coronal reformatted contrast-enhanced CT scan demonstrated no evidence of subcapsular hepatic hematoma or perihepatic free air, suggesting liver perforation.
Reference
-
1. Aliperti G. Complications related to diagnostic and therapeutic endoscopic retrograde cholangiopancreatography. Gastrointest Endosc Clin N Am. 1996; 6:379–407.2. Hart R, Classen M. Complications of diagnostic gastrointestinal endoscopy. Endoscopy. 1990; 22:229–233.3. Enns R, Eloubeidi MA, Mergener K, Jowell PS, Branch MS, Pappas TM, et al. ERCP-related perforations: risk factors and management. Endoscopy. 2002; 34:293–298.4. Del Pozo D, Moral I, Poves E, Sanz C, Martín M. Subcapsular hepatic hematoma following ERCP: case report and review. Endoscopy. 2011; 43:Suppl 2 UCTN. E164–E165.5. Dupas JL, Mancheron H, Sevenet F, Delamarre J, Delcenserie R, Capron JP. Hepatic subcapsular biloma. An unusual complication of endoscopic retrograde cholangiopancreatography. Gastroenterology. 1988; 94(5 Pt 1):1225–1227.6. Kayashima H, Ikegami T, Kasagi Y, Hidaka G, Yamazaki K, Sadanaga N, et al. Liver Parenchyma Perforation following Endoscopic Retrograde Cholangiopancreatography. Case Rep Gastroenterol. 2011; 5:487–491.7. Kawakami H, Kuwatani M, Kudo T, Ehira N, Yamato H, Asaka M. Portobiliary fistula: unusual complication of wire-guided cannulation during endoscopic retrograde cholangiopancreatography. Endoscopy. 2011; 43:Suppl 2 UCTN. E98–E99.8. Ferreira LE, Baron TH. Post-sphincterotomy bleeding: who, what, when, and how. Am J Gastroenterol. 2007; 102:2850–2858.9. Green MH, Duell RM, Johnson CD, Jamieson NV. Haemobilia. Br J Surg. 2001; 88:773–786.10. Srivastava DN, Sharma S, Pal S, Thulkar S, Seith A, Bandhu S, et al. Transcatheter arterial embolization in the management of hemobilia. Abdom Imaging. 2006; 31:439–448.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hemobilia due to arteriobiliary fistula complicating ERCP for residual bile duct stone in a case of Mirizzi syndrome
- Successful Treatment of an Iatrogenic Hepatic Arteriobiliary Fistula with an Endobiliary Covered Stent Graft: A Case Report
- Portal cavernography during endoscopic retrograde cholangiopancreatography: from bilhemia to hemobilia
- Four Cases of Guidewire Induced Periampullary Perforation During Endoscopic Retrograde Cholangiopancreatography
- Subcapsular Hepatic Hematoma after Endoscopic Retrograde Cholangiopancreatography
