Effectiveness of Mechanical Embolectomy for Septic Embolus in the Cerebral Artery Complicated with Infective Endocarditis
- Affiliations
-
- 1Department of Internal Medicine, Jeju National University School of Medicine, Jeju, Korea. neosangtaek@naver.com
- 2Department of Neurosurgery, Jeju National University School of Medicine, Jeju, Korea.
- KMID: 1793033
- DOI: http://doi.org/10.3346/jkms.2013.28.8.1244
Abstract
- There has been a controversy over data of thrombolytic and endovascular surgical treatment about cerebral infarction secondary to infective endocarditis. We report a woman who received early mechanical embolectomy as a treatment of acute stroke with infective endocarditis. A 35-yr-old woman was hospitalized due to right hemiparesis. Brain image showed cerebral infarction at the middle cerebral artery and echocardiography demonstrated vegetation at the mitral valve. She was successfully treated with embolectomy and parenteral antibiotics without any neurologic sequelae. This report shows that the early retrieve of septic cerebral emboli can be a helpful treatment of acute stroke associated with endocarditis.
MeSH Terms
-
Adult
Anti-Bacterial Agents/therapeutic use
Cerebral Arteries/radiography/*surgery
Embolectomy
Endocarditis/complications/*diagnosis/drug therapy
Female
Humans
Intracranial Embolism/surgery
Mitral Valve/ultrasonography
Streptococcus/isolation & purification
Stroke/*diagnosis/etiology/surgery
Tomography, X-Ray Computed
Anti-Bacterial Agents
Figure
-

Fig. 1 The change of signal intensity of the left middle cerebral artery in brain magnetic resonance image (MRI). (A) MRI shows hyperintensity in diffusion-weighted image (arrow). (B) The image shows perfusion delay in mean transit time. (C) Time to peak maps of the left middle cerebral artery territory shows diffusion-perfusion mismatch.
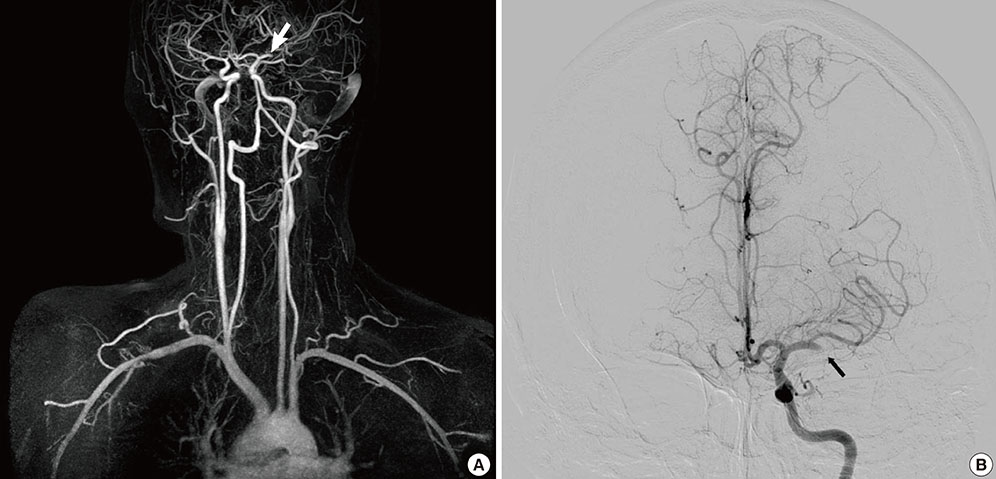
Fig. 2 Angiographic findings of cerebral flow. (A) Magnetic resonance angiography shows stopping of left middle cerebral artery (arrow). (B) Left internal cerebral artery angiography reveals abrupt cessation of left proximal middle cerebral flow (arrow).

Fig. 3 Left internal cerebral artery angiography shows recanalization of middle cerebral artery after mechanical intra-arterial embolectomy.

Fig. 4 Retrievable solitaire stent and captured emboli are shown (arrows).
Cited by 1 articles
-
Forced Arterial Suction Thrombectomy of Septic Embolic Middle Cerebral Artery Occlusion Due to Infective Endocarditis: an Illustrative Case and Review of the Literature
Jeong-Min Kim, Ji-Su Jeon, Yong-Won Kim, Dong-Hun Kang, Yang-Ha Hwang, Yong-Sun Kim
Neurointervention. 2014;9(2):101-105. doi: 10.5469/neuroint.2014.9.2.101.
Reference
-
1. Baddour LM, Wilson WR, Bayer AS, Fowler VG Jr, Bolger AF, Levison ME, Ferrieri P, Gerber MA, Tani LY, Gewitz MH, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation. 2005; 111:e394–e434.2. Walker KA, Sampson JB, Skalabrin EJ, Majersik JJ. Clinical Characteristics and Thrombolytic Outcomes of Infective Endocarditis-Associated Stroke. Neurohospitalist. 2012; 2:87–91.3. Kan P, Webb S, Siddiqui AH, Levy EI. First reported use of retrievable stent technology for removal of a large septic embolus in the middle cerebral artery. World Neurosurg. 2012; 77:591.e1–591.e5.4. Sukumaran S, Jayadevan ER, Mandilya A, Sreedharan SE, Harikrishnan S, Radhakrishnan N, Sylaja PN. Successful mechanical thrombectomy of acute middle cerebral artery occlusion due to vegetation from infective endocarditis. Neurol India. 2012; 60:239–240.5. Dababneh H, Hedna VS, Ford J, Taimeh Z, Peters K, Mocco J, Waters MF. Endovascular intervention for acute stroke due to infective endocarditis: case report. Neurosurg Focus. 2012; 32:E1.6. Higashida RT, Furlan AJ, Roberts H, Tomsick T, Connors B, Barr J, Dillon W, Warach S, Broderick J, Tilley B, et al. Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke. 2003; 34:e109–e137.7. Bhuva P, Kuo SH, Claude Hemphill J, Lopez GA. Intracranial hemorrhage following thrombolytic use for stroke caused by infective endocarditis. Neurocrit Care. 2010; 12:79–82.8. Heiro M, Nikoskelainen J, Engblom E, Kotilainen E, Marttila R, Kotilainen P. Neurologic manifestations of infective endocarditis: a 17-year experience in a teaching hospital in Finland. Arch Intern Med. 2000; 160:2781–2787.9. Jenkinson HF, Lamont RJ. Oral microbial communities in sickness and in health. Trends Microbiol. 2005; 13:589–595.10. Douglas CW, Heath J, Hampton KK, Preston FE. Identity of viridans streptococci isolated from cases of infective endocarditis. J Med Microbiol. 1993; 39:179–182.11. Ruttmann E, Willeit J, Ulmer H, Chevtchik O, Höfer D, Poewe W, Laufer G, Müller LC. Neurological outcome of septic cardioembolic stroke after infective endocarditis. Stroke. 2006; 37:2094–2099.12. Sila C. Anticoagulation should not be used in most patients with stroke with infective endocarditis. Stroke. 2011; 42:1797–1798.13. Gillinov AM, Shah RV, Curtis WE, Stuart RS, Cameron DE, Baumgartner WA, Greene PS. Valve replacement in patients with endocarditis and acute neurologic deficit. Ann Thorac Surg. 1996; 61:1125–1129.14. Kang DH, Kim YJ, Kim SH, Sun BJ, Kim DH, Yun SC, Song JM, Choo SJ, Chung CH, Song JK, et al. Early surgery versus conventional treatment for infective endocarditis. N Engl J Med. 2012; 366:2466–2473.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mechanical Thrombectomy for Septic Embolism Secondary to Staphylococcus lugdunensis Bacteremia without Infective Endocarditis: A Case Report
- Sudden Cardiac Death Caused by a Septic Coronary Artery Embolism as the First Clinical Presentation of Infective Endocarditis
- A case of acute myocardial infarction caused by a septic coronary embolism and treated with embolectomy
- Forced Arterial Suction Thrombectomy of Septic Embolic Middle Cerebral Artery Occlusion Due to Infective Endocarditis: an Illustrative Case and Review of the Literature
- A Case of Cerebral Mycotic Aneurysm Complicated with Subarachnoid Hemorrhage due to Infective Endocarditis
