Ketonuria after Fasting may be Related to the Metabolic Superiority
- Affiliations
-
- 1Department of Family Practice and Community Health, Ajou University School of Medicine, Suwon, Korea.
- 2Department of Family Medicine, CHA Biomedical Center, CHA University College of Medicine, Seoul, Korea. kosso@chollian.net
- KMID: 1792902
- DOI: http://doi.org/10.3346/jkms.2010.25.12.1771
Abstract
- Obese individuals are less able to oxidize fat than non-obese individuals. Caloric reduction or fasting can detect ketonuria. We investigated the differences of metabolic parameters in the presence of ketonuria after a minimum 8 hr fast in a cross-sectional analysis of 16,523 Koreans (6,512 women and 10,011 men). The relationship between the presence of ketonuria of all subjects and prevalence of obesity, central obesity, metabolic syndrome, and obesity-related metabolic parameters were assessed. The ketonuria group had lower prevalence of obesity, central obesity, and metabolic syndrome than the non-ketonuria group. In addition, all metabolic parameters (including body weight, waist circumference, blood glucose, high-density lipoprotein, triglyceride, blood pressure, and insulin) were favorable in the ketonuria group than in the non-ketonuria group, even after adjustment for age, tobacco use, and alcohol consumption. The odds ratios of having obesity (odds ratio [OR]=1.427 in women, OR=1.582 in men, P<0.05), central obesity (OR=1.675 in women, OR=1.889 in men, P<0.05), and metabolic syndrome (OR=3.505 in women, OR=1.356 in men, P<0.05) were increased in the non-ketonuria group compared to the ketonuria group. The presence of ketonuria after at least an 8 hr fast may be indicative of metabolic superiority.
Keyword
MeSH Terms
-
Blood Glucose/analysis
Blood Pressure
Body Weight
Cross-Sectional Studies
*Fasting
Female
Humans
Insulin/blood
Ketosis/*complications/diagnosis
Lipoproteins, HDL/blood
Male
Metabolic Syndrome X/*complications/epidemiology
Obesity/complications/epidemiology
Odds Ratio
Time Factors
Triglycerides/blood
Waist Circumference
Figure
-
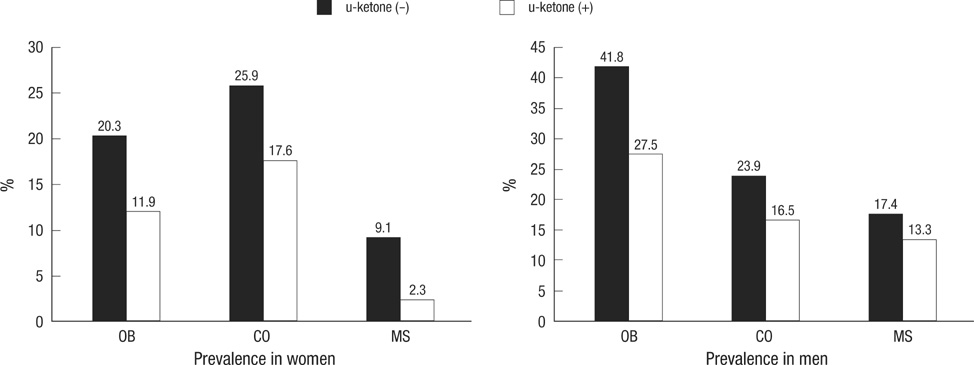
Fig. 1 Prevalence of obesity, central obesity, and metabolic syndrome according to the presence of ketonuria in all subjects. This figure is representing the prevalence of obesity, central obesity, and metabolic syndrome according to the presence of ketonuria and all showed statistically significant difference (P<0.05) in both genders. OB, obesity (body mass index ≥25.0 kg/m2); CO, central obesity (men ≥90 cm, women ≥85 cm); MS, metabolic syndrome followed by NCEP-ATP III.

Fig. 2 Prevalence of obesity, central obesity, and metabolic syndrome in each generation. This figure shows the prevalence of obesity, central obesity, and metabolic syndrome from the 20th to the 50th in both genders according to ketonuria under overnight fasting condition, which may represent that all subjects with ketonuria under fasting condition could be more metabolic benefit compared to the non-ketonuria. *P<0.05 in each generation in both genders.
Cited by 2 articles
-
The Presence of Urinary Ketones according to Metabolic Status and Obesity
Bo-Reum Kim, Jeong Woo Seo, Sang Man Kim, Kyu-Nam Kim, Nam-Seok Joo
J Korean Med Sci. 2020;35(31):e273. doi: 10.3346/jkms.2020.35.e273.Evaluation of the Clinical Significance of Ketonuria
Hae-Won Jung, Ile-Kyu Park
Lab Med Online. 2012;2(1):15-19. doi: 10.3343/lmo.2012.2.1.3.
Reference
-
1. Paek KW, Chun KH, Lee KW. Relationship between metabolic syndrome and familial history of hypertension/stroke, diabetes, and cardiovascular disease. J Korean Med Sci. 2006. 21:701–708.
Article2. Snijder MB, Zimmet PZ, Visser M, Dekker JM, Seidell JC, Shaw JE. Independent and opposite associations of waist and hip circumferences with diabetes, hypertension and dyslipidemia: the AusDiab Study. Int J Obes Relat Metab Disord. 2004. 28:402–409.
Article3. Snijder MB, Dekker JM, Visser M, Bouter LM, Stehouwer CD, Kostense PJ, Yudkin JS, Heine RJ, Nijpels G, Seidell JC. Associations of hip and thigh circumferences independent of waist circumference with the incidence of type 2 diabetes: the Hoorn Study. Am J Clin Nutr. 2003. 77:1192–1197.
Article4. Seidell JC, Pérusse L, Després JP, Bouchard C. Waist and hip circumferences have independent and opposite effects on cardiovascular disease risk factors: the Quebec Family Study. Am J Clin Nutr. 2001. 74:315–321.
Article5. Jeong SK, Kim YK, Park JW, Shin YJ, Kim DS. Impact of visceral fat on metabolic syndrome and nonalcoholic liver diseases. J Korean Med Sci. 2008. 23:789–795.6. Bigaard J, Frederiksen K, Tjønneland A, Thomsen BL, Overvad K, Heitmann BL, Sørensen TI. Waist and hip circumferences and all-cause mortality: usefulness of the waist-to-hip ratio? Int J Obes Relat Metab Disord. 2004. 28:741–747.
Article7. Jee SH, Sull JW, Park J, Lee SY, Ohrr H, Guallar E, Samet JM. Body mass index and mortality in Korean men and women. N Engl J Med. 2006. 355:779–787.8. Fantuzzi G. Adipose tissue, adipokines, and inflammation. J Allergy Clin Immunol. 2005. 115:911–919.
Article9. Hsieh CH, Hung YJ, Wu DA, Kuo SW, Lee CH, Sheu WH, Li JC, Yeh KH, Chen CY, Pei D. Impact of Clinical Characteristics of Individual Metabolic Syndrome on the Severity of Insulin Resistance in Chinese Adults. J Korean Med Sci. 2007. 22:74–80.
Article10. Gianotti TF, Sookoian S, Dieuzeide G, García SI, Gemma C, González CD, Pirola CJ. A decreased mitochondrial DNA content is related to insulin resistance in adolescents. Obesity (Silver Spring). 2008. 16:1591–1595.
Article11. Beisswenger BG, Delucia EM, Lapoint N, Sanford RJ, Beisswenger PJ. Ketosis leads to increased methylglyoxal production on the Atkins diet. Ann N Y Acad Sci. 2005. 1043:201–210.
Article12. Musa-Veloso K, Likhodii SS, Cunnane SC. Breath acetone is a reliable indicator of ketosis in adults consuming ketogenic meals. Am J Clin Nutr. 2002. 76:65–70.
Article13. Shah P, Isley WL. Ketoacidosis during a low-carbohydrate diet. N Engl J Med. 2006. 354:97–98.
Article14. Mohammadiha H. Resistance to ketonuria and ketosis in obese subjects. Am J Clin Nutr. 1974. 27:1212–1213.
Article15. Opie LH, Walfish PG. Plasma free fatty acid concentrations in obesity. N Engl J Med. 1963. 268:757–760.
Article16. Gordon JE, Chitkara ID, Wyon JB. Weanling diarrhea. Am J Med Sci. 1963. 245:345–377.
Article17. Astrup A, Meinert Larsen T, Harper A. Atkins and other low-carbohydrate diets: hoax or an effective tool for weight loss? Lancet. 2004. 364:897–899.
Article18. National Institutes of Health. National Heart, Lung, and Blood Institute and the North American Association of the Study of Obesity. NIH publication number 00-4084. The practical guide: identification, evaluation and treatment of overweight and obesity in adults. 2000.19. Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, Kim DY, Kwon HS, Kim SR, Lee CB, Oh SJ, Park CY, Yoo HJ. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract. 2007. 75:72–80.
Article20. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA. 2001. 285:2486–2497.21. Nordmann AJ, Nordmann A, Briel M, Keller U, Yancy WS Jr, Brehm BJ, Bucher HC. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Arch Intern Med. 2006. 166:285–293.22. Gardner CD, Kiazand A, Alhassan S, Kim S, Stafford RS, Balise RR, Kraemer HC, King AC. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial. JAMA. 2007. 297:969–977.
Article23. Foster GD, Wyatt HR, Hill JO, McGuckin BG, Brill C, Mohammed BS, Szapary PO, Rader DJ, Edman JS, Klein S. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med. 2003. 348:2082–2090.
Article24. Tendler D, Lin S, Yancy WS Jr, Mavropoulos J, Sylvestre P, Rockey DC, Westman EC. The effect of a low-carbohydrate, ketogenic diet on nonalcoholic fatty liver disease: a pilot study. Dig Dis Sci. 2007. 52:589–593.
Article25. Shai I, Schwarzfuchs D, Henkin Y, Shahar DR, Witkow S, Greenberg I, Golan R, Fraser D, Bolotin A, Vardi H, Tangi-Rozental O, Zuk-Ramot R, Sarusi B, Brickner D, Schwartz Z, Sheiner E, Marko R, Katorza E, Thiery J, Fiedler GM, Blüher M, Stumvoll M, Stampfer MJ. Dietary Intervention Randomized Controlled Trial (DIRECT) Group. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med. 2008. 359:229–241.
Article26. Erlanson-Albertsson C, Mei J. The effect of low carbohydrate on energy metabolism. Int J Obes (Lond). 2005. 29:Suppl 2. S26–S30.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Different Response of Body Weight Change According to Ketonuria after Fasting in the Healthy Obese
- The Presence of Urinary Ketones according to Metabolic Status and Obesity
- Evaluation of the Clinical Significance of Ketonuria
- Urine Organic Acid Analysis of Patients with Febrile Seizures
- Clinical Significance of Fasting Glucose Criteria in Metabolic Syndrome
