The Presence of Urinary Ketones according to Metabolic Status and Obesity
- Affiliations
-
- 1Department of Family Practice and Community Health, Ajou University School of Medicine, Suwon, Korea
- 2Functional Medicine Clinic, Green Cross I-Med (GCIMED), Seoul, Korea
- KMID: 2505199
- DOI: http://doi.org/10.3346/jkms.2020.35.e273
Abstract
- Background
Recently, new concepts about obesity and normal weight subtypes with metabolic conditions are rising and ketone bodies are emerging as a significant indicator of metabolic health. This study aimed to find a relationship between ketonuria and those subtypes.
Methods
The data of 19,036 subjects were analyzed in this cross-sectional study (2013–2017 Korea National Health and Nutrition Examination Survey, KNHANES). Based on body mass index and adult treatment panel III with modification of waist circumference, individuals were categorized into 4 groups: metabolically healthy normal weight (MHNW), metabolically healthy obese (MHO), metabolically unhealthy normal weight (MUNW), and metabolically unhealthy obese (MUO). Individuals were divided into 2 groups, positive and negative ketonuria groups, and the metabolic parameters were compared.
Results
The metabolic indicators of the positive ketonuria group showed better results than those of the negative ketonuria group and the MHNW group showed the highest proportion of positive ketonuria. The MHNW group showed higher urinary ketones than the MUO group (odds ratio [OR], 0.391; 95% confidence interval [CI], 0.254–0.601) in men. In women, OR of having ketonuria was 0.698 (95% CI, 0.486–1.002) in the MHO group and 0.467 (95% CI, 0.226–0.966) in the MUNW group compared to the MHNW group, respectively.
Conclusion
Compared to the MHNW group, the MUO group showed lower presence of ketonuria in men, and tendency to have less ketonuria in women.
Keyword
Figure
-
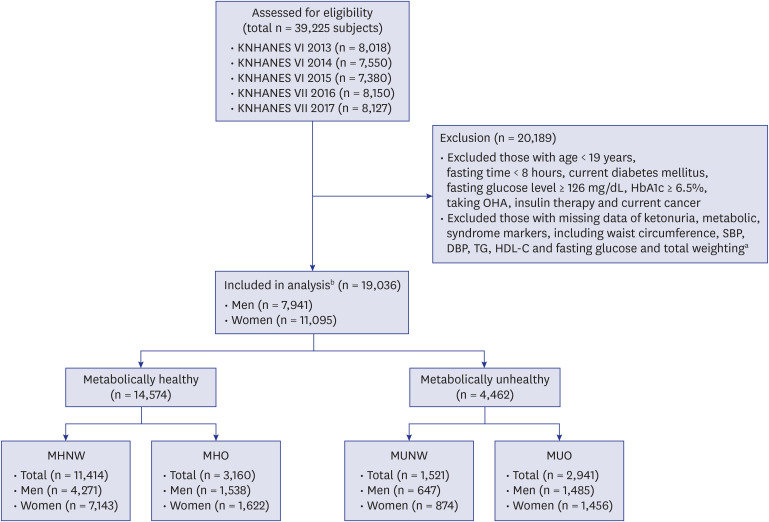
Fig. 1 Flowchart showing the selection and categorization of study subjects.KNHANES = Korean National Health and Nutrition Examination Survey, BMI = body mass index, HbA1c = glycated hemoglobin, OHA = oral hypoglycemic agent, SBP = systolic blood pressure, DBP = diastolic blood pressure, TG = triglyceride, HDL-C = high-density lipoprotein-cholesterol, MHNW = metabolically healthy normal weight, MHO = metabolically healthy obese, MUNW = metabolically unhealthy normal weight, MUO = metabolically unhealthy obese.aData from health interview, health examination and nutritional survey; bSubjects who did not meet the inclusion and exclusion criteria were not eliminated. Individuals who met all the inclusion and exclusion criteria were regarded as the analysis group.
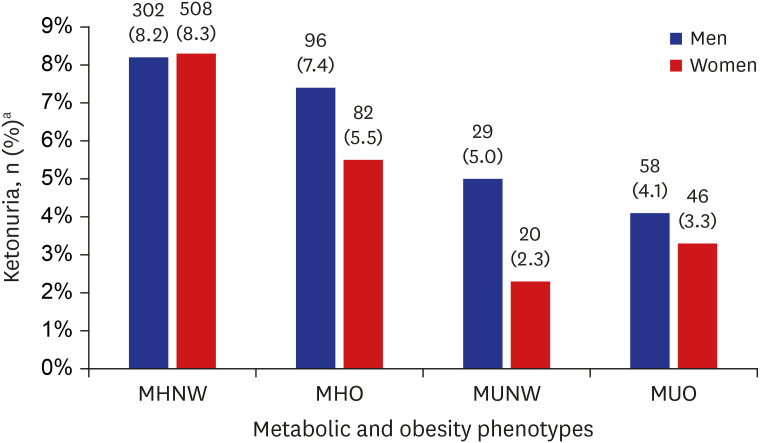
Fig. 2 Proportion of ketonuria in each metabolic and obesity phenotype.P value < 0.001 both in men and women; P value is calculated by χ2 test under complex sample analysis.MHNW = metabolically healthy normal weight, MHO = metabolically healthy obese, MUNW = metabolically unhealthy normal weight, MUO = metabolically unhealthy obese.aValues are presented as unweighted number (weighted %).
Reference
-
1. Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, et al. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA. 2003; 289(1):76–79. PMID: 12503980.
Article2. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004; 364(9438):937–952. PMID: 15364185.
Article4. Bray GA. Medical consequences of obesity. J Clin Endocrinol Metab. 2004; 89(6):2583–2589. PMID: 15181027.
Article5. World Health Organization. Obesity and overweight [Internet]. Updated 2020. Accessed January 20, 2020. https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweigh.6. Stefan N, Häring HU, Hu FB, Schulze MB. Metabolically healthy obesity: epidemiology, mechanisms, and clinical implications. Lancet Diabetes Endocrinol. 2013; 1(2):152–162. PMID: 24622321.
Article7. Stefan N, Häring HU, Schulze MB. Metabolically healthy obesity: the low-hanging fruit in obesity treatment? Lancet Diabetes Endocrinol. 2018; 6(3):249–258. PMID: 28919065.
Article8. Stefan N, Kantartzis K, Machann J, Schick F, Thamer C, Rittig K, et al. Identification and characterization of metabolically benign obesity in humans. Arch Intern Med. 2008; 168(15):1609–1616. PMID: 18695074.
Article9. Wildman RP, Muntner P, Reynolds K, McGinn AP, Rajpathak S, Wylie-Rosett J, et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999-2004). Arch Intern Med. 2008; 168(15):1617–1624. PMID: 18695075.
Article10. Ruderman N, Chisholm D, Pi-Sunyer X, Schneider S. The metabolically obese, normal-weight individual revisited. Diabetes. 1998; 47(5):699–713. PMID: 9588440.
Article11. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation. 2005; 112(17):2735–2752. PMID: 16157765.12. Owen OE, Morgan AP, Kemp HG, Sullivan JM, Herrera MG, Cahill GF Jr. Brain metabolism during fasting. J Clin Invest. 1967; 46(10):1589–1595. PMID: 6061736.
Article13. Owen OE, Felig P, Morgan AP, Wahren J, Cahill GF Jr. Liver and kidney metabolism during prolonged starvation. J Clin Invest. 1969; 48(3):574–583. PMID: 5773093.
Article14. Joo NS, Lee DJ, Kim KM, Kim BT, Kim CW, Kim KN, et al. Ketonuria after fasting may be related to the metabolic superiority. J Korean Med Sci. 2010; 25(12):1771–1776. PMID: 21165293.
Article15. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004; 363(9403):157–163. PMID: 14726171.16. Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract. 2007; 75(1):72–80. PMID: 16735075.
Article17. Brant LC, Wang N, Ojeda FM, LaValley M, Barreto SM, Benjamin EJ, et al. Relations of metabolically healthy and unhealthy obesity to digital vascular function in three community-based cohorts: a meta-analysis. J Am Heart Assoc. 2017; 6(3):e004199. PMID: 28275071.
Article18. Wildman RP, Muntner P, Reynolds K, McGinn AP, Rajpathak S, Wylie-Rosett J, et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999–2004). Arch Intern Med. 2008; 168(15):1617–1624. PMID: 18695075.
Article19. Caleyachetty R, Thomas GN, Toulis KA, Mohammed N, Gokhale KM, Balachandran K, et al. Metabolically healthy obese and incident cardiovascular disease events among 3.5 million men and women. J Am Coll Cardiol. 2017; 70(12):1429–1437. PMID: 28911506.20. Chen HH, Tseng YJ, Wang SY, Tsai YS, Chang CS, Kuo TC, et al. The metabolome profiling and pathway analysis in metabolic healthy and abnormal obesity. Int J Obes. 2015; 39(8):1241–1248.
Article21. Dobson R, Burgess MI, Sprung VS, Irwin A, Hamer M, Jones J, et al. Metabolically healthy and unhealthy obesity: differential effects on myocardial function according to metabolic syndrome, rather than obesity. Int J Obes. 2016; 40(1):153–161.
Article22. Eckel N, Li Y, Kuxhaus O, Stefan N, Hu FB, Schulze MB. Transition from metabolic healthy to unhealthy phenotypes and association with cardiovascular disease risk across BMI categories in 90 257 women (the Nurses' Health Study): 30 year follow-up from a prospective cohort study. Lancet Diabetes Endocrinol. 2018; 6(9):714–724. PMID: 29859908.
Article23. Kim G, Lee SG, Lee BW, Kang ES, Cha BS, Ferrannini E, et al. Spontaneous ketonuria and risk of incident diabetes: a 12 year prospective study. Diabetologia. 2019; 62(5):779–788. PMID: 30788528.24. Kim HJ, Joo NS, Kim KM, Lee DJ, Kim SM. Different response of body weight change according to ketonuria after fasting in the healthy obese. J Korean Med Sci. 2012; 27(3):250–254. PMID: 22379334.
Article25. Mohammadiha H. Resistance to ketonuria and ketosis in obese subjects. Am J Clin Nutr. 1974; 27(11):1212–1213. PMID: 4447089.
Article26. Newman JC, Verdin E. Ketone bodies as signaling metabolites. Trends Endocrinol Metab. 2014; 25(1):42–52. PMID: 24140022.
Article27. Rodríguez JC, Gil-Gómez G, Hegardt FG, Haro D. Peroxisome proliferator-activated receptor mediates induction of the mitochondrial 3-hydroxy-3-methylglutaryl-CoA synthase gene by fatty acids. J Biol Chem. 1994; 269(29):18767–18772. PMID: 7913466.
Article28. Bae KH, Kim JG, Park KG. Transcriptional regulation of fibroblast growth factor 21 expression. Endocrinol Metab (Seoul). 2014; 29(2):105–111. PMID: 25031882.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Impact of Exercise on the Presence of Urinary Ketones Based on Korea National Health and Nutrition Examination Survey Data, 2014–2015
- Journal of Obesity & Metabolic Syndrome: A New International Journal Targeting the Pathophysiology and Treatment of Obesity and Metabolic Syndrome
- The Influence of Obesity and Metabolic Health on Vascular Health
- Obesity Defined by Body Mass Index and Metabolic Status in the Elderly
- Vitamin D and Metabolic Diseases: Growing Roles of Vitamin D
