Iliocaval Fistula Presenting with Paradoxical Pulmonary Embolism Combined with High-Output Heart Failure Successfully Treated by Endovascular Stent-Graft Repair: Case Report
- Affiliations
-
- 1Cardiovascular Center and Division of Cardiology, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea. kyoonseok@catholic.ac.kr
- 2Divison of Vascular Surgery, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea.
- 3Divison of Interventional Radiology, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea.
- KMID: 1789992
- DOI: http://doi.org/10.3346/jkms.2014.29.2.296
Abstract
- A 51-yr-old man presented exertional dyspnea as a consequence of iliocaval fistula combined with paradoxical pulmonary embolism and high-output heart failure. Endovascular stent-graft repair was performed to cover iliocaval fistula and restore the heart function. After the procedure, dyspnea was improved and procedure related complication was not seen. A 6-month follow-up computed tomography showed regression of pulmonary thromboembolism and well-positioned stent-graft without graft migration, aortacaval communication or endoleak. Stent graft implantation should be considered an alternative of open repair surgery for treament of abdominal arteriovenous fisula, especially in patient with high risk for surgery.
MeSH Terms
Figure
-

Fig. 1 Contrast-enhanced abdominal CT images. (A-C) Images at diagnosis showed 40×38 mm sized right iliac artery aneurysm and iliocaval fistula (black arrow) with thrombus (white arrows). (D-F) Follow-up images at 6 months after endovascular stent-graft repair demonstrated patency of the graft, without evidence of graft migration or aortocaval communication. (A, D) Transverse veiw; (B) Coronal view; (C) Sagittal view; (E) Coronal maximal intensity projection view; (F) Sagittal maximal intensity projection view.
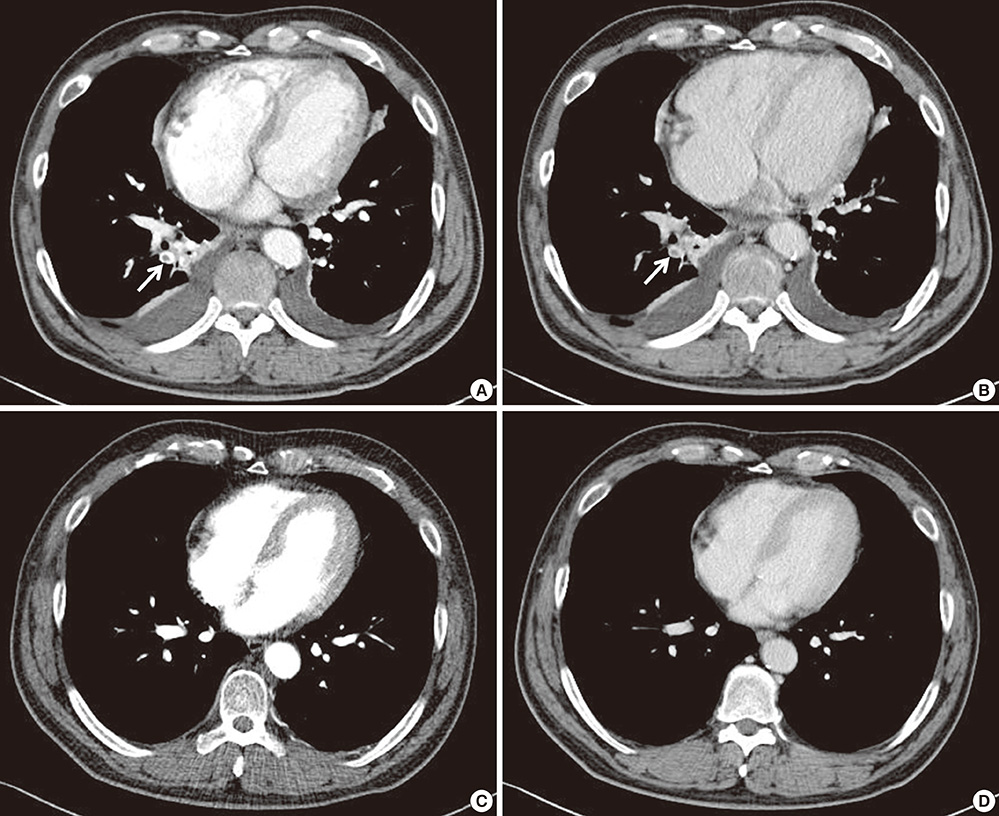
Fig. 2 Contrast-enhanced chest CT images. (A, B) Images at diagnosis showed pulmonary thromboembolism (arrows) that involved right lower lobe base segmental pulmonary artery. (C, D) Follow-up chest CT scans at 6 months after coumadization showed much regressed pulmonary embolism. (A, C) Arterial phase; (B, D) Venous phase.

Fig. 3 Angiography findings. (A) Embolization of right common iliac artery was performed with PLUG 10 mm (dotted arrow). (B) Pelvic arteriogram showed aneurysmal dilatation of right common iliac artery, iliocaval shunt and some filling defects near the aneurysm (white arrow indicate thrombus). (C) Angiography after deployment of the stents showed well implanted graft stents and no visible of IVC.
Reference
-
1. Gilling-Smith GL, Mansfield AO. Spontaneous abdominal arteriovenous fistulae: report of eight cases and review of the literature. Br J Surg. 1991; 78:421–425.2. Lim RP, Stella DL, Dowling RJ, Campbell WA, Hebbard GS. Iliocaval arteriovenous fistula presenting with multiple organ failure. Australas Radiol. 2006; 50:381–385.3. De Rango P, Parlani G, Cieri E, Verzini F, Isernia G, Silvestri V, Cao P. Paradoxical pulmonary embolism with spontaneous aortocaval fistula. Ann Vasc Surg. 2012; 26:739–746.4. Schmidt R, Bruns C, Walter M, Erasmi H. Aorto-caval fistula--an uncommon complication of infrarenal aortic aneurysms. Thorac Cardiovasc Surg. 1994; 42:208–211.5. Rajmohan B. Spontaneous aortocaval fistula. J Postgrad Med. 2002; 48:203–205.6. Leigh-Smith S, Smith RC. Aorto caval fistula: the "bursting heart syndrome". J Accid Emerg Med. 2000; 17:223–225.7. Antoniou GA, Koutsias S, Karathanos C, Sfyroeras GS, Vretzakis G, Giannoukas AD. Endovascular stent-graft repair of major abdominal arteriovenous fistula: a systematic review. J Endovasc Ther. 2009; 16:514–523.8. Cheung A, Shuman WP, Kohler TR. Diagnosis by computed tomography of arteriovenous fistula complicating ruptured iliac artery aneurysm. J Vasc Surg. 1987; 6:605–608.9. Brewster DC, Cambria RP, Moncure AC, Darling RC, LaMuraglia GM, Geller SC, Abbott WM. Aortocaval and iliac arteriovenous fistulas: recognition and treatment. J Vasc Surg. 1991; 13:253–264.10. Melas N, Saratzis A, Abbas A, Sarris K, Saratzis N, Lazaridis I, Kiskinis D. Endovascular repair of a spontaneous ilio-iliac fistula presenting as pulmonary embolism. Vasa. 2011; 40:246–250.11. Woolley DS, Spence RK. Aortocaval fistula treated by aortic exclusion. J Vasc Surg. 1995; 22:639–642.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular stent-graft repair of aortocaval fistula complicated by the rupture of abdominal aortic aneurysm
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- A Case of Impending Paradoxical Embolus in a Patient with Acute Pulmonary Embolism
- Congenital Intracranial Pial Arteriovenous Fistula Complicated with Congestive Heart Failure in Neonate: A Case Report
- A case of aortobronchial fistula caused by thoracic aortic aneurysm and successfully treated with an endovascular stent graft
