The Clinical Feasibility of Using Non-Breath-Hold Real-Time MR-Echo Imaging for the Evaluation of Mediastinal and Chest Wall Tumor Invasion
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine and the Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul 110-744, Korea. jmgoo@plaza.snu.ac.kr
- 2Seoul National University Hospital, Healthcare Gangnam Center, Seoul 135-984, Korea.
- 3Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Cancer Research Institute, Seoul National University College of Medicine, Seoul 110-744, Korea.
- KMID: 1787012
- DOI: http://doi.org/10.3348/kjr.2010.11.1.37
Abstract
OBJECTIVE
We wanted to determine the clinical feasibility of using non-breath-hold real-time MR-echo imaging for the evaluation of mediastinal and chest wall tumor invasion.
MATERIALS AND METHODS
MR-echo imaging was prospectively applied to 45 structures in 22 patients who had non-small cell lung cancer when the tumor invasion was indeterminate on CT. The static MR imaging alone, and the static MR imaging combined with MR-echo examinations were analyzed. The surgical and pathological findings were compared with using the Wilcoxon-signed rank test and McNemar's test.
RESULTS
The accuracy, sensitivity and specificity of the combined MR-echo examination and static MR imaging for determining the presence of invasion were 84%, 83% and 85%, respectively, for the first reading session and they were 87%, 83% and 87%, respectively, for the second reading session (there was substantial interobserver agreement, k = 0.74). For the static MR imaging alone, these values were 62%, 83% and 59%, respectively, for the first reader and they were 69%, 67% and 74%, respectively, for the second reader (there was moderate interobserver agreement, k = 0.49). The diagnostic confidence for tumor invasion was also higher for the combined MR-echo examination and static MR imaging than that for the static MR imaging alone (p < 0.05).
CONCLUSION
The combined reading of a non-breath-hold real-time MR-echo examination and static MR imaging provides higher specificity and diagnostic confidence than those for the static MR imaging reading alone to determine the presence of mediastinal or chest wall tumor invasion when this was indeterminate on CT scanning.
MeSH Terms
Figure
-
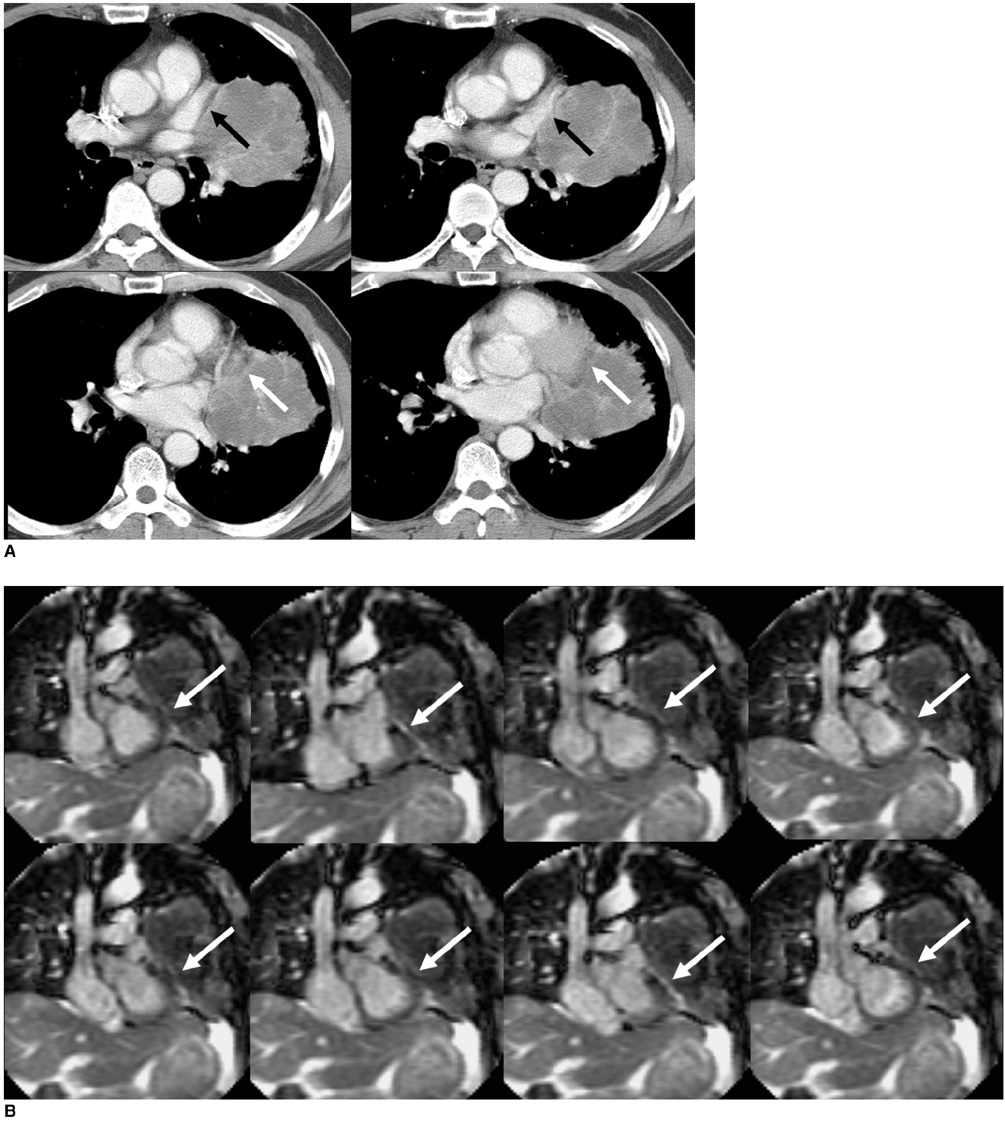
Fig. 1 Positive sliding sign in 54-year-old man with lung cancer. A. On CT images, fat plane loss and wide contact with left ventricle and atrial appendage (arrows) were observed. B. Non-breath hold real-time MR-echo image showing sliding sign at left atrial appendage and left ventricle. Note high signal intensity of normal pericardial fluid (white arrows) between mass and left ventricle. No invasion of left atrial appendage or ventricle was observed.

Fig. 2 Positive sliding sign in 73-year-old man with lung cancer. A. On CT images, mass encased descending aorta over 90 degrees and mass obstructed left lower lobar bronchus (white arrows). B. Non-breath-hold real-time MR-echo image showing mass sliding upwards (white arrow) over descending aorta on expiration. Left lower lobectomy was performed and no aortic invasion by mass was found during subsequent pathologic examination.
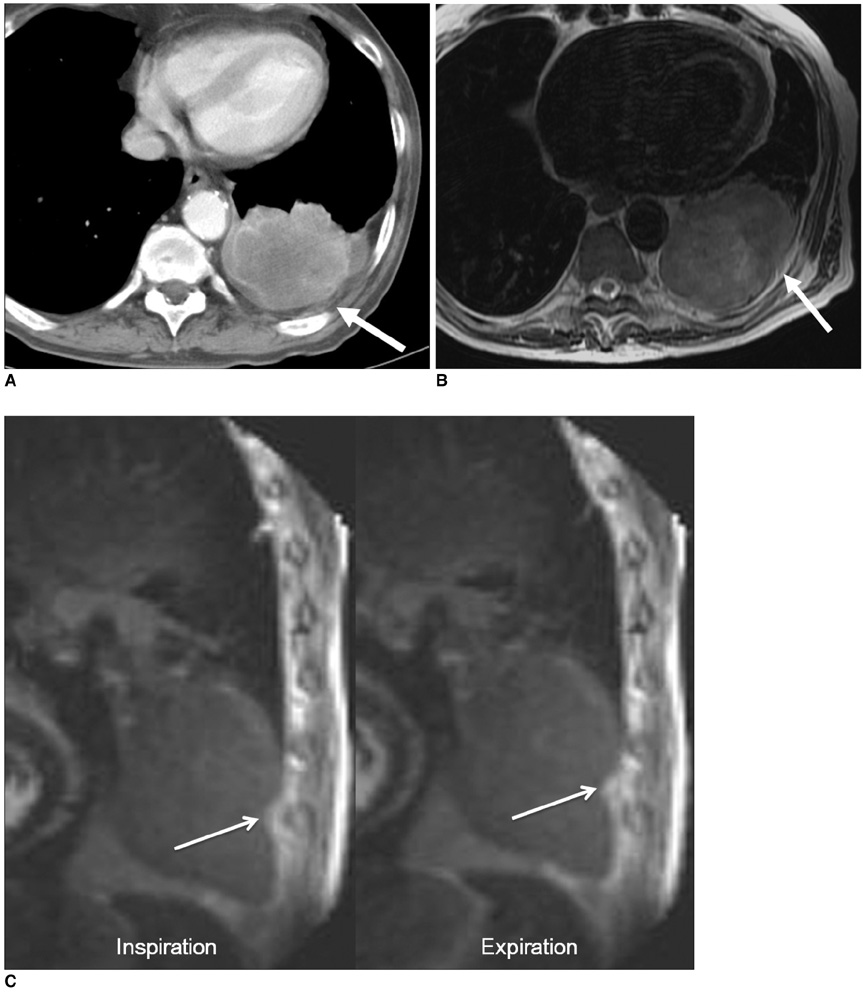
Fig. 3 Positive sliding sign in 71-year-old man with lung cancer. A, B. On CT (A), and axial fast spin-echo MR (B) images show suspicious fat obliteration and wide contact (arrows) between mass and chest wall in lower lobe. C. Sagittal MR-echo examination inspiratory and expiratory images show sliding sign or movement over posterior chest wall (white arrows). Surgeon could be confident before operation that mass could be safely removed without en-bloc resection of chest wall. There was no invasion to parietal pleura or chest wall on pathologic examination after operation.
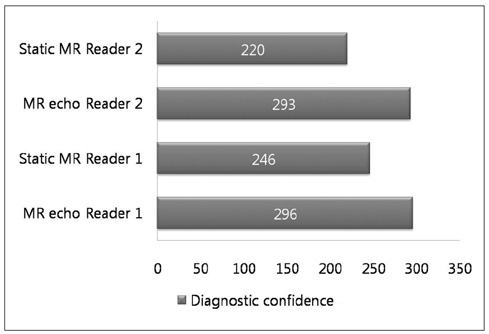
Fig. 4 Diagnostic confidence scores were assessed for two readers. For both readers, diagnostic confidence score was significantly higher for combined MR echo and static MR images than that for static MR images alone (Reader 1 and 2: p < 0.05).
Reference
-
1. Albertucci M, DeMeester TR, Rothberg M, Hagen JA, Santoscoy R, Smyrk TC. Surgery and the management of peripheral lung tumors adherent to the parietal pleura. J Thorac Cardiovasc Surg. 1992. 103:8–12.2. Downey RJ, Martini N, Rusch VW, Bains MS, Korst RJ, Ginsberg RJ. Extent of chest wall invasion and survival in patients with lung cancer. Ann Thorac Surg. 1999. 68:188–193.3. Pairolero PC. Extended resections for lung cancer. How far is too far? Eur J Cardiothorac Surg. 1999. 16:S48–S50.4. Mansour KA, Thourani VH, Losken A, Reeves JG, Miller JI Jr, Carlson GW, et al. Chest wall resections and reconstruction: a 25-year experience. Ann Thorac Surg. 2002. 73:1720–1725.5. Glazer HS, Duncan-Meyer J, Aronberg DJ, Moran JF, Levitt RG, Sagel SS. Pleural and chest wall invasion in bronchogenic carcinoma: CT evaluation. Radiology. 1985. 157:191–194.6. Webb WR, Gatsonis C, Zerhouni EA, Heelan RT, Glazer GM, Francis IR, et al. CT and MR imaging in staging non-small cell bronchogenic carcinoma: report of the Radiologic Diagnostic Oncology Group. Radiology. 1991. 178:705–713.7. White PG, Adams H, Crane MD, Butchart EG. Preoperative staging of carcinoma of the bronchus: can computed tomographic scanning reliably identify stage III tumours? Thorax. 1994. 49:951–957.8. Venuta F, Rendina EA, Ciriaco P, Polettini E, Di Biasi C, Gualdi GF, et al. Computed tomography for preoperative assessment of T3 and T4 bronchogenic carcinoma. Eur J Cardiothorac Surg. 1992. 6:238–241.9. Herman SJ, Winton TL, Weisbrod GL, Towers MJ, Mentzer SJ. Mediastinal invasion by bronchogenic carcinoma: CT signs. Radiology. 1994. 190:841–846.10. Kauczor HU, Plathow C. Imaging tumour motion for radiotherapy planning using MRI. Cancer Imaging. 2006. 6:S140–S144.11. Ohno Y, Adachi S, Motoyama A, Kusumoto M, Hatabu H, Sugimura K, et al. Multiphase ECG-triggered 3D contrast-enhanced MR angiography: utility for evaluation of hilar and mediastinal invasion of bronchogenic carcinoma. J Magn Reson Imaging. 2001. 13:215–224.12. Haage P, Piroth W, Krombach G, Karaagac S, Schaffter T, Gunther RW, et al. Pulmonary embolism: comparison of angiography with spiral computed tomography, magnetic resonance angiography, and real-time magnetic resonance imaging. Am J Respir Crit Care Med. 2003. 167:729–734.13. Plathow C, Klopp M, Schoebinger M, Thieke C, Fink C, Puderbach M, et al. Monitoring of lung motion in patients with malignant pleural mesothelioma using two-dimensional and three-dimensional dynamic magnetic resonance imaging: comparison with spirometry. Invest Radiol. 2006. 41:443–448.14. Sakai S, Murayama S, Murakami J, Hashiguchi N, Masuda K. Bronchogenic carcinoma invasion of the chest wall: evaluation with dynamic cine MRI during breathing. J Comput Assist Tomogr. 1997. 21:595–600.15. Seo JS, Kim YJ, Choi BW, Choe KO. Usefulness of magnetic resonance imaging for evaluation of cardiovascular invasion: evaluation of sliding motion between thoracic mass and adjacent structures on cine MR images. J Magn Reson Imaging. 2005. 22:234–241.16. Takahashi K, Furuse M, Hanaoka H, Yamada T, Mineta M, Ono H, et al. Pulmonary vein and left atrial invasion by lung cancer: assessment by breath-hold gadolinium-enhanced three-dimensional MR angiography. J Comput Assist Tomogr. 2000. 24:557–561.17. Lim HK, Kim S, Lim JH, Kim SH, Lee WJ, Chun H, et al. Assessment of pancreatic invasion in patients with advanced gastric carcinoma: usefulness of the sliding sign on sonograms. AJR Am J Roentgenol. 1999. 172:615–618.18. Lim JH, Ko YT, Lee DH. Sonographic sliding sign in localization of right upper quadrant mass. J Ultrasound Med. 1990. 9:455–459.19. Kodalli N, Erzen C, Yuksel M. Evaluation of parietal pleural invasion of lung cancers with breathhold inspiration and expiration MRI. Clin Imaging. 1999. 23:227–235.20. Glazer HS, Kaiser LR, Anderson DJ, Molina PL, Emami B, Roper CL, et al. Indeterminate mediastinal invasion in bronchogenic carcinoma: CT evaluation. Radiology. 1989. 173:37–42.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Non-Breath-Hold T2-weighted Turbo Spin-Echo and Three Breath-Hold T2-weighted MR Images for Detection of Focal Hepatic Lesion
- Single breath-hold MR imaging of liver
- Breath-Hold MR Imaging of Focal Hepatic Lesions: Clinical Usefulness of Breath-Hold TSE T2WI Combined by FastLow-Angle Shot (FLASH) MR Imaging
- Optimal MR Pulse Sequences for Hepatic Hemangiomas: Comparison of T2-Weighted Turbo-Spin-Echo, T2-Weighted Breath-hold Turbo-Spin-Echo, and T1-Weighted FLASH Dynamic Imaging
- Role of EPI in Diagnosing Cavernous Hemangioma & Small HCC: Comparision with Fast T2-Weighted MR Imaging
