Solitary Fibrous Tumor Arising from Stomach: CT Findings
- Affiliations
-
- 1Department of Diagnostic Radiology, Severance Hospital and Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea. kimnex@yuhs.ac
- 2Institute of Gastroenterology and Brain Korea 21 Project for Medical Science, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Severance Hospital and Research Institute of Pathological Science, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1786226
- DOI: http://doi.org/10.3349/ymj.2007.48.6.1056
Abstract
- Solitary fibrous tumors are spindle-cell neoplasms that usually develop in the pleura and peritoneum, and rarely arise in the stomach. To our knowledge, there is only one case reporting a solitary fibrous tumor arising from stomach in the English literature. Here we report the case of a 26-year-old man with a large solitary fibrous tumor arising from the stomach which involved the submucosa and muscular layer and resembled a gastrointestinal stromal tumor in the stomach, based on what was seen during abdominal computed tomography. A solitary fibrous tumor arising from the stomach, although rare, could be considered as a diagnostic possibility for gastric submucosal tumors.
Keyword
MeSH Terms
Figure
-
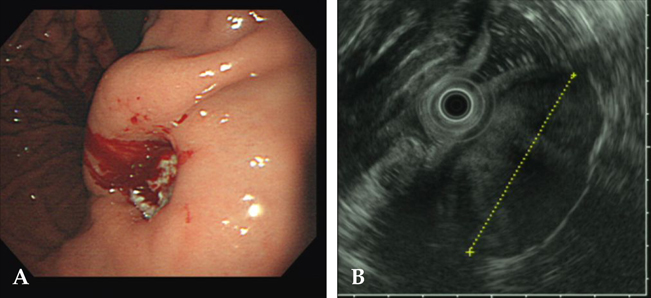
Fig. 1 (A) Endoscopy showed a large submucosal tumor in the gastric body with bleeding from a large central ulceration that contained fluid and residual contrast material from a previous barium study. (B) Endoscopic ultrasound (EUS) also showed a large submucosal mass in the gastric body portion.

Fig. 2 Abdominal computed tomography (CT) demonstrated about 5.5 × 3.2 cm sized, well defined large mass arising from the posterior aspect of the lesser curvature side of the gastric body. (A) The mass showed relative hypoattenuation on the precontrast images. (B) In the portal phase, the mass showed intense heterogeneous enhancement. Ulceration in the luminal side and low attenuation in the central cavity were seen within the mass. (C) In the equilibrium phase, the mass showed prolonged enhancement and the bulk of the tumor was seen in an extragastric location.
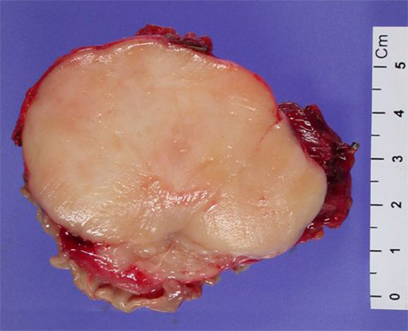
Fig. 3 On gross pathology, the specimen was an ovoid, lobulated solid mass, measuring 5.4 × 5.2 × 4 cm, which was attached to the stomach as a portion of the stomach. On sectioning of the specimen, it was a well demarcated and relatively homogeneously yellowish mass involving submucosa and muscular layer.
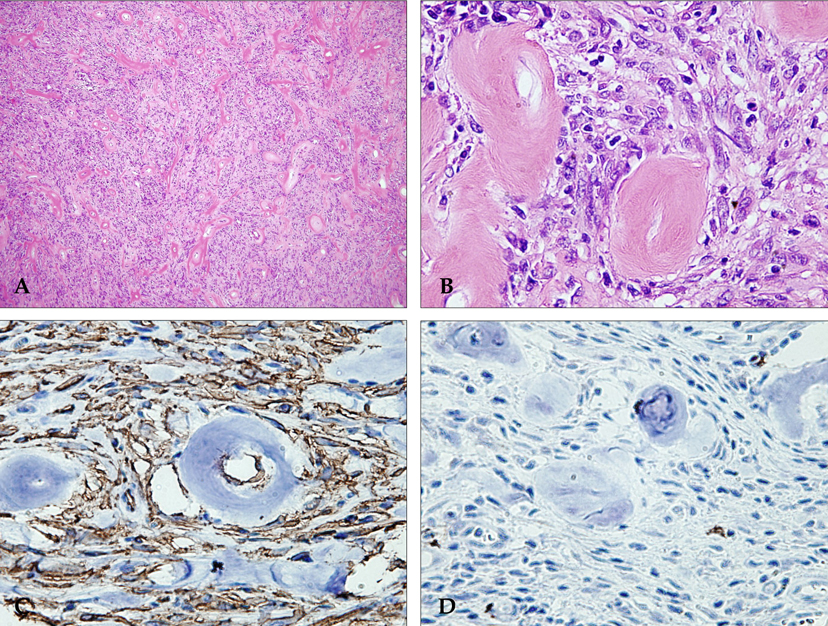
Fig. 4 Histologic findings by Hematoxylin and Eosin [H-E] stains (A, B) and immunohistochemical findings for CD34 and c-kit. (C, D). (A) Photomicrograph (original magnification, × 100; H-E stain) shows that the patternless proliferation of spindle cells with abundant perivascular and intercellular mature collagen formation. Dilated, thick-walled vessels were common in the lesions. (B) High power photomicrograph (original magnification, × 400; H-E stain) shows that non-atypical, round to spindle-shaped tumor cells have little cytoplasm with indistinct borders and dispersed chromatin within vesicular nuclei. There was rarely mitosis. (C, D) The tumor cells showed strong immunoreactivity characteristic of neoplastic cells for CD34 (immunoperoxidase, × 400) (C) and the tumor was negative for c-kit (× 400) (D).
Reference
-
1. Gold JS, Antonescu CR, Hajdu C, Ferrone CR, Hussain M, Lewis JJ, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002. 94:1057–1068.2. Vossough A, Torigian DA, Zhang PJ, Siegelman ES, Banner MP. Extrathoracic solitary fibrous tumor of the pelvic peritoneum with central malignant degeneration on CT and MRI. J Magn Reson Imaging. 2005. 22:684–686.3. Shidham VB, Weiss JP, Quinn TJ, Grotkowski CE. Fine needle aspiration cytology of gastric solitary fibrous tumor: a case report. Acta Cytol. 1998. 42:1159–1166.4. Kindblom LG, Remotti HE, Aldenborg F, Meis-Kindblom JM. Gastrointestinal pacemaker cell tumor (GIPACT): gastrointestinal stromal tumors show phenotypic characteristics of the interstitial cells of Cajal. Am J Pathol. 1998. 152:1259–1269.5. Lee WA, Lee MK, Jeen YM, Kie JH, Chung JJ, Yun SH. Solitary fibrous tumor arising in gastric serosa. Pathol Int. 2004. 54:436–439.6. Rosado-de-Christenson ML, Abbott GF, McAdams HP, Franks TJ, Galvin JR. From the archives of the AFIP: Localized fibrous tumor of the pleura. Radiographics. 2003. 23:759–783.7. Goodlad JR, Fletcher CD. Solitary fibrous tumour arising at unusual sites: analysis of a series. Histopathology. 1991. 19:515–522.8. Fukunaga M, Naganuma H, Ushigome S, Endo Y, Ishikawa E. Malignant solitary fibrous tumour of the peritoneum. Histopathology. 1996. 28:463–466.9. Hasegawa T, Matsuno Y, Shimoda T, Hasegawa F, Sano T, Hirohashi S. Extrathoracic solitary fibrous tumors: their histological variability and potentially aggressive behavior. Hum Pathol. 1999. 30:1464–1473.10. Levy AD, Remotti HE, Thompson WM, Sobin LH, Miettinen M. Gastrointestinal stromal tumors: radiologic features with pathologic correlation. Radiographics. 2003. 23:283–304. 456; quiz 532.11. Horton KM, Juluru K, Montogomery E, Fishman EK. Computed tomography imaging of gastrointestinal stromal tumors with pathology correlation. J Comput Assist Tomogr. 2004. 28:811–817.12. McLeod AJ, Zornoza J, Shirkhoda A. Leiomyosarcoma: computed tomographic findings. Radiology. 1984. 152:133–136.13. Pannu HK, Hruban RH, Fishman EK. CT of gastric leiomyosarcoma: patterns of involvement. AJR Am J Roentgenol. 1999. 173:369–373.14. Horton KM, Fishman EK. Current role of CT in imaging of the stomach. Radiographics. 2003. 23:75–87.15. Dunfee BL, Sakai O, Spiegel JH, Pistey R. Solitary fibrous tumor of the buccal space. AJNR Am J Neuroradiol. 2005. 26:2114–2116.16. Miettinen M, Virolainen M, Maarit-Sarlomo-Rikala . Gastrointestinal stromal tumors--value of CD34 antigen in their identification and separation from true leiomyomas and schwannomas. Am J Surg Pathol. 1995. 19:207–216.17. Sarlomo-Rikala M, Kovatich AJ, Barusevicius A, Miettinen M. CD117: a sensitive marker for gastrointestinal stromal tumors that is more specific than CD34. Mod Pathol. 1998. 11:728–734.18. Fukunaga M, Naganuma H, Nikaido T, Harada T, Ushigome S. Extrapleural solitary fibrous tumor: a report of seven cases. Mod Pathol. 1997. 10:443–450.19. Vallat-Decouvelaere AV, Dry SM, Fletcher CD. Atypical and malignant solitary fibrous tumors in extrathoracic locations: evidence of their comparability to intra-thoracic tumors. Am J Surg Pathol. 1998. 22:1501–1511.20. Lowbeer L. Hypoglycemia-producing extrapancreatic neoplasms. A review. Am J Clin Pathol. 1961. 35:233–243.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imaging Findings of a Solitary Fibrous Tumor in Pancreas: A Case Report
- Solitary Fibrous Tumor of the Adrenal Gland: A Case Report
- An Ancillary CT Finding of Intrapulmonary Solitary Fibrous Tumor: A Case Report
- A case of solitary fibrous tumor arising from the vagina
- Solitary Fibrous Tumor of the Trachea: CT Findings with a Pathological Correlation
